This chapter discusses microscopic examination of urine sediment. It describes how to prepare urine samples for microscopic analysis and examine them under a microscope. The document outlines normal and abnormal urine sediments including red blood cells, white blood cells, epithelial cells, casts, crystals, and bacteria. It provides clinical significance of findings and how to standardize reporting. Proper collection and examination of urine sediment can provide valuable information for diagnosing urinary tract disorders.
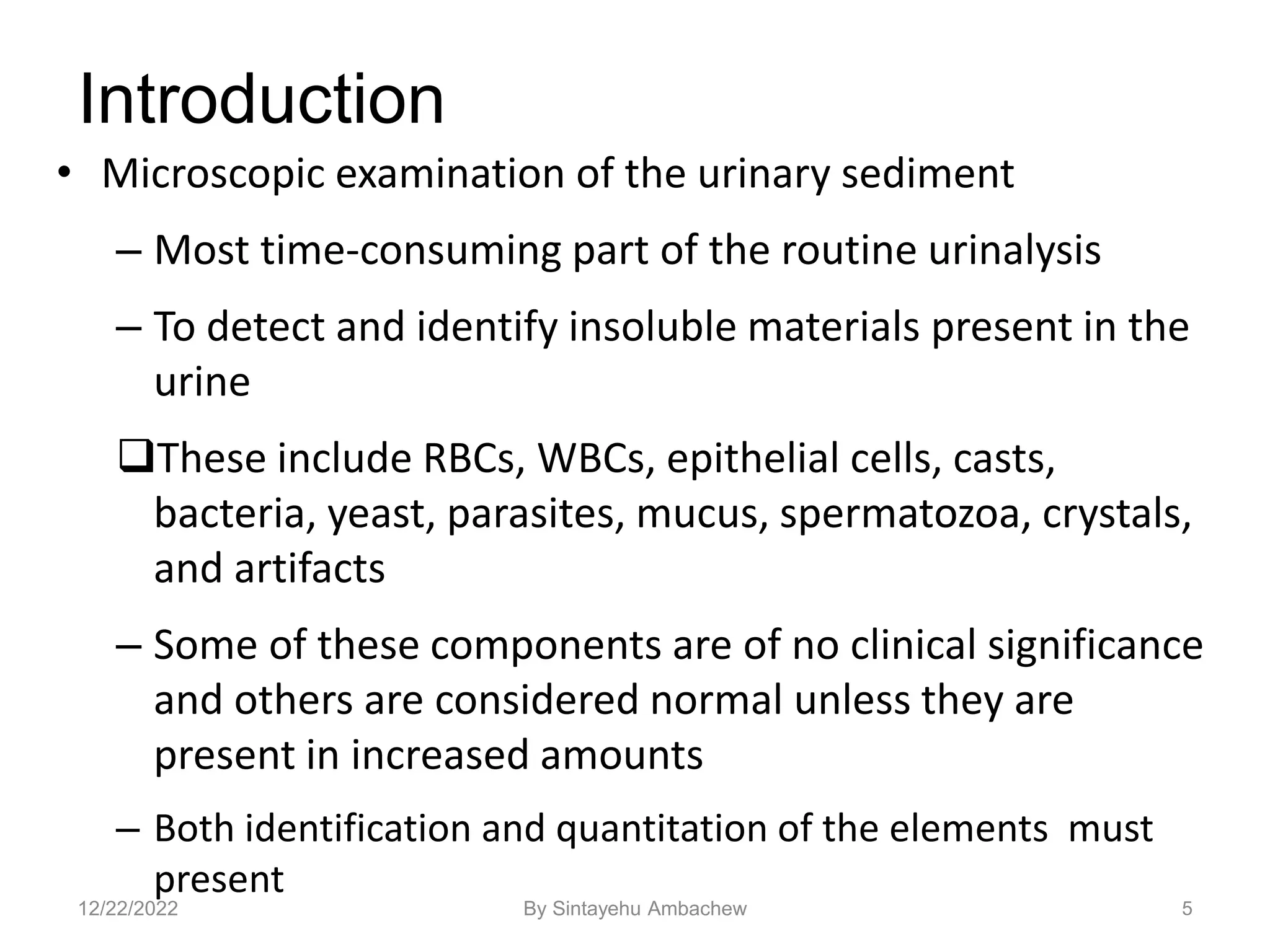
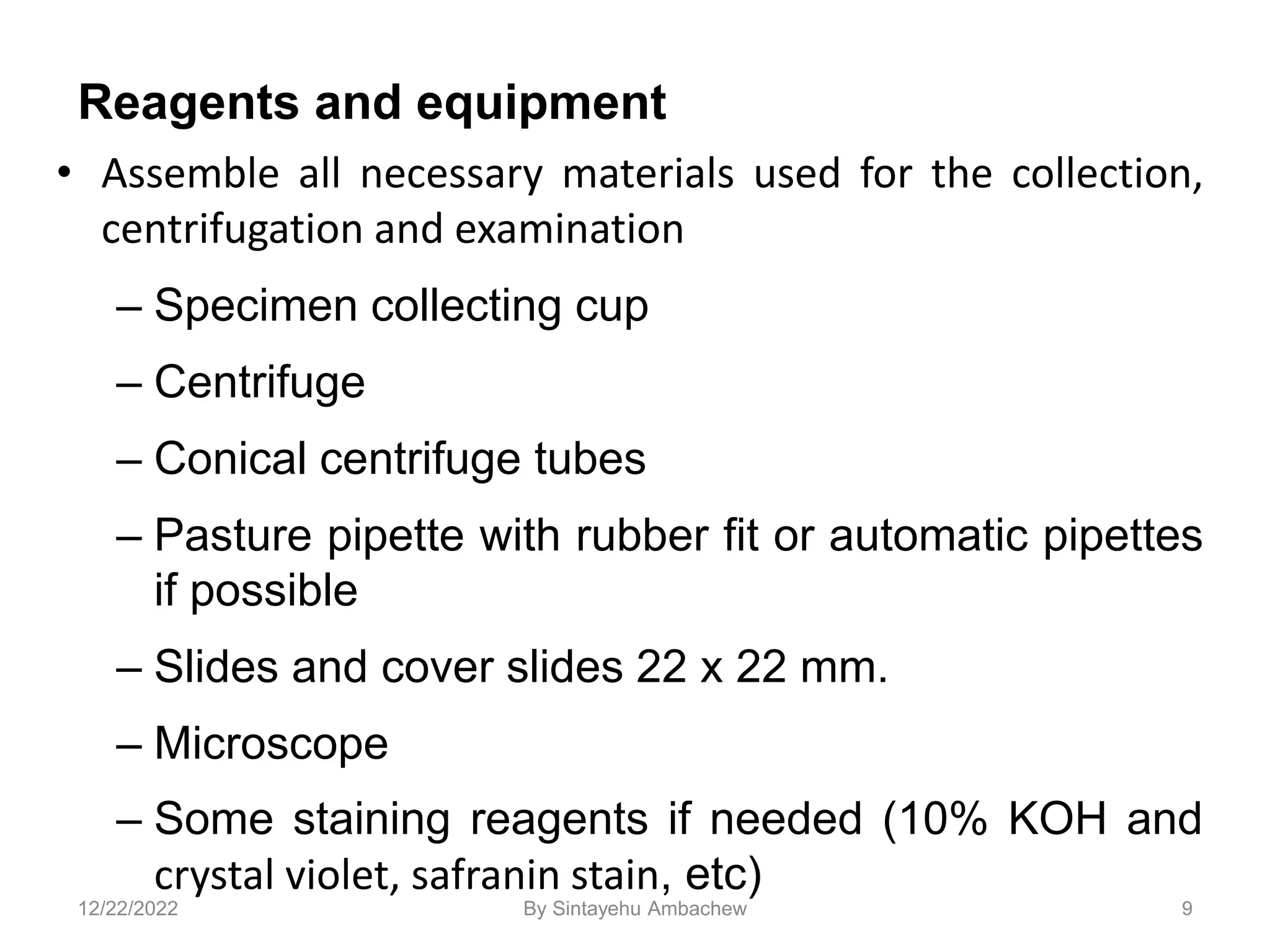
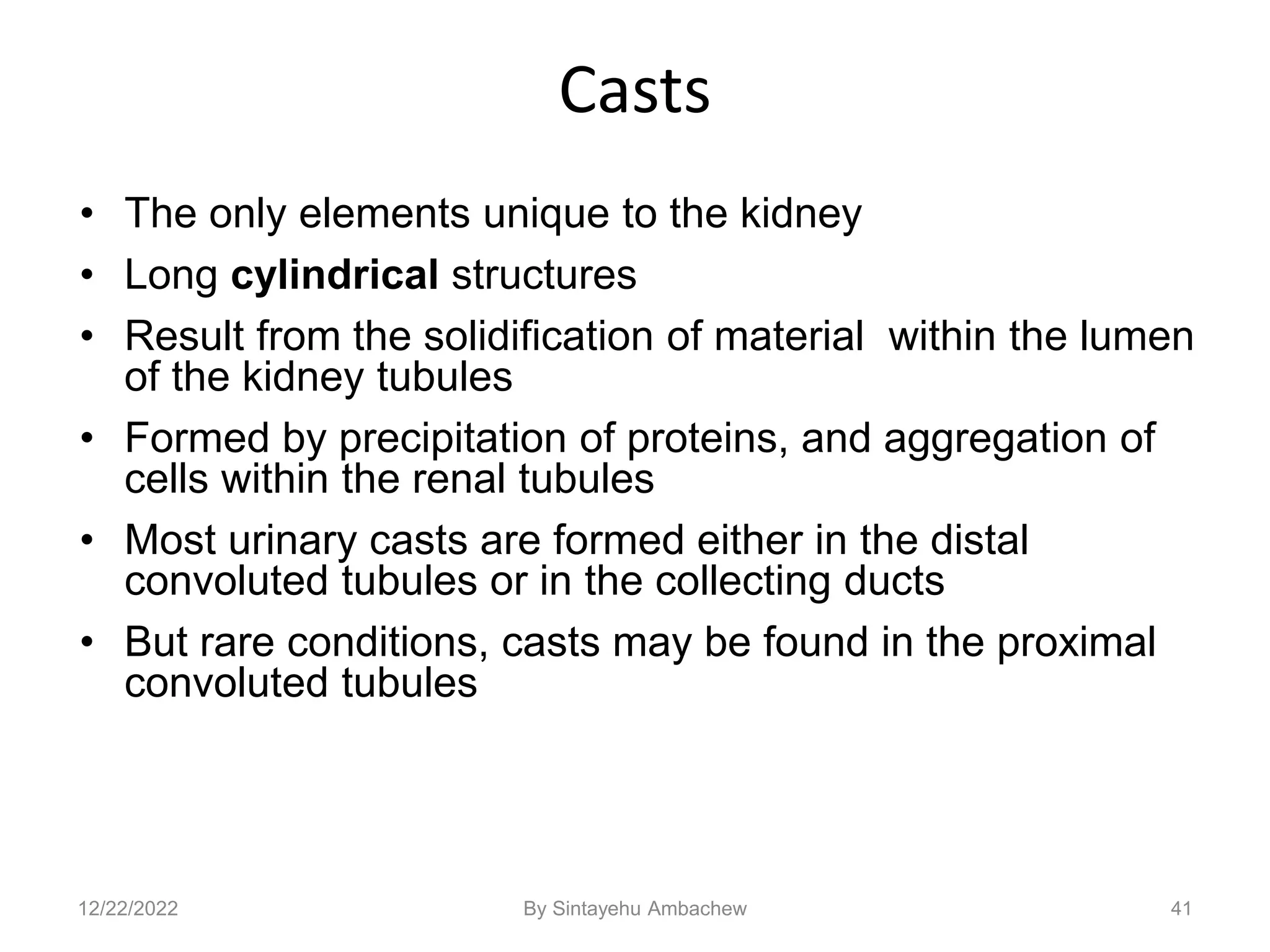


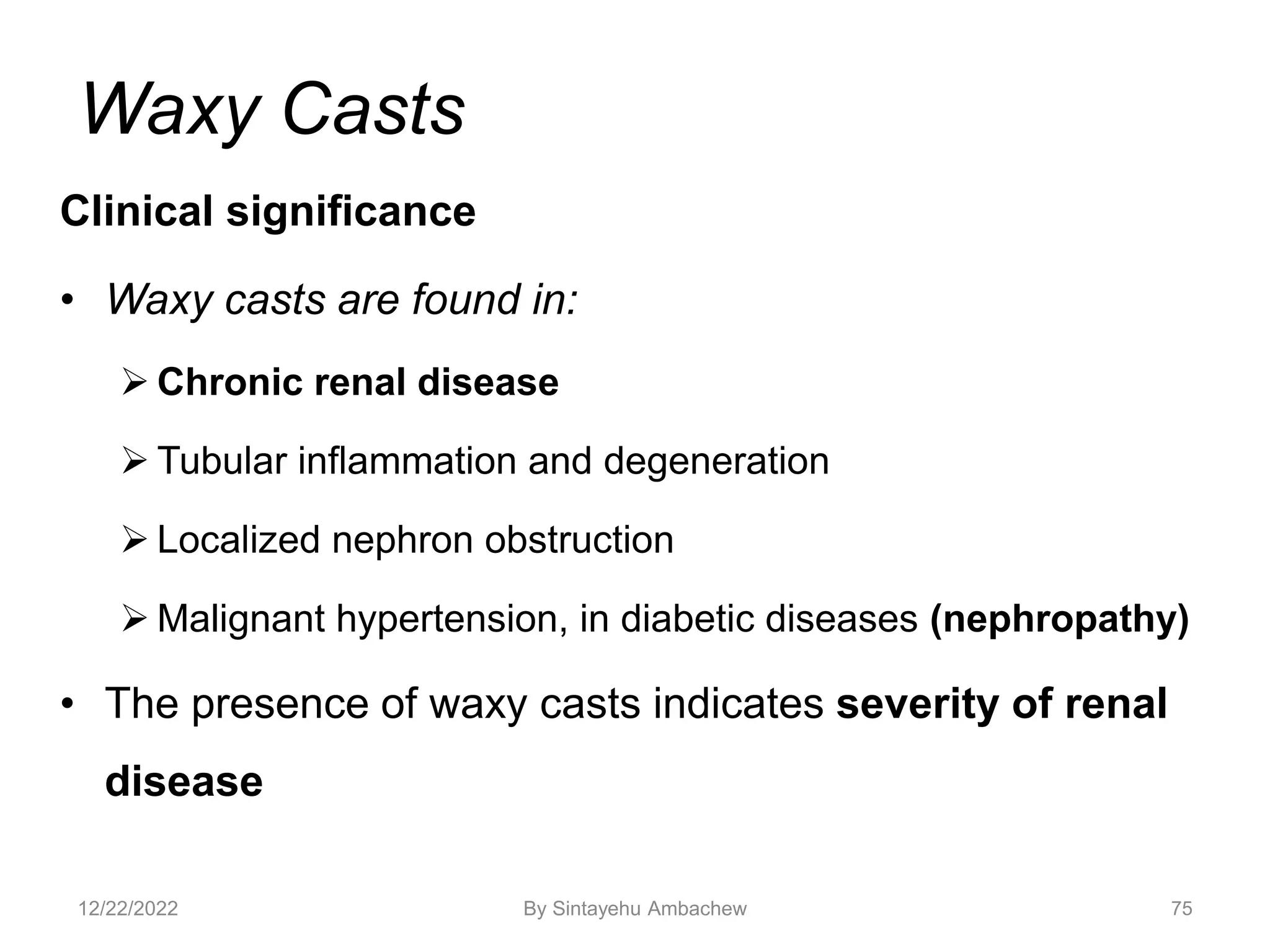
![• This is a cast
containing ‘fat’
bodies, high
power
• On wet mount
the droplets are
highly refractile
[they bounce the
light back]
77
12/22/2022 By Sintayehu Ambachew](https://image.slidesharecdn.com/microscopicexaminationofurinesediments-221222023650-c3614b1d/75/Microscopic-examination-of-Urine-sediments-ppt-77-2048.jpg)


![122
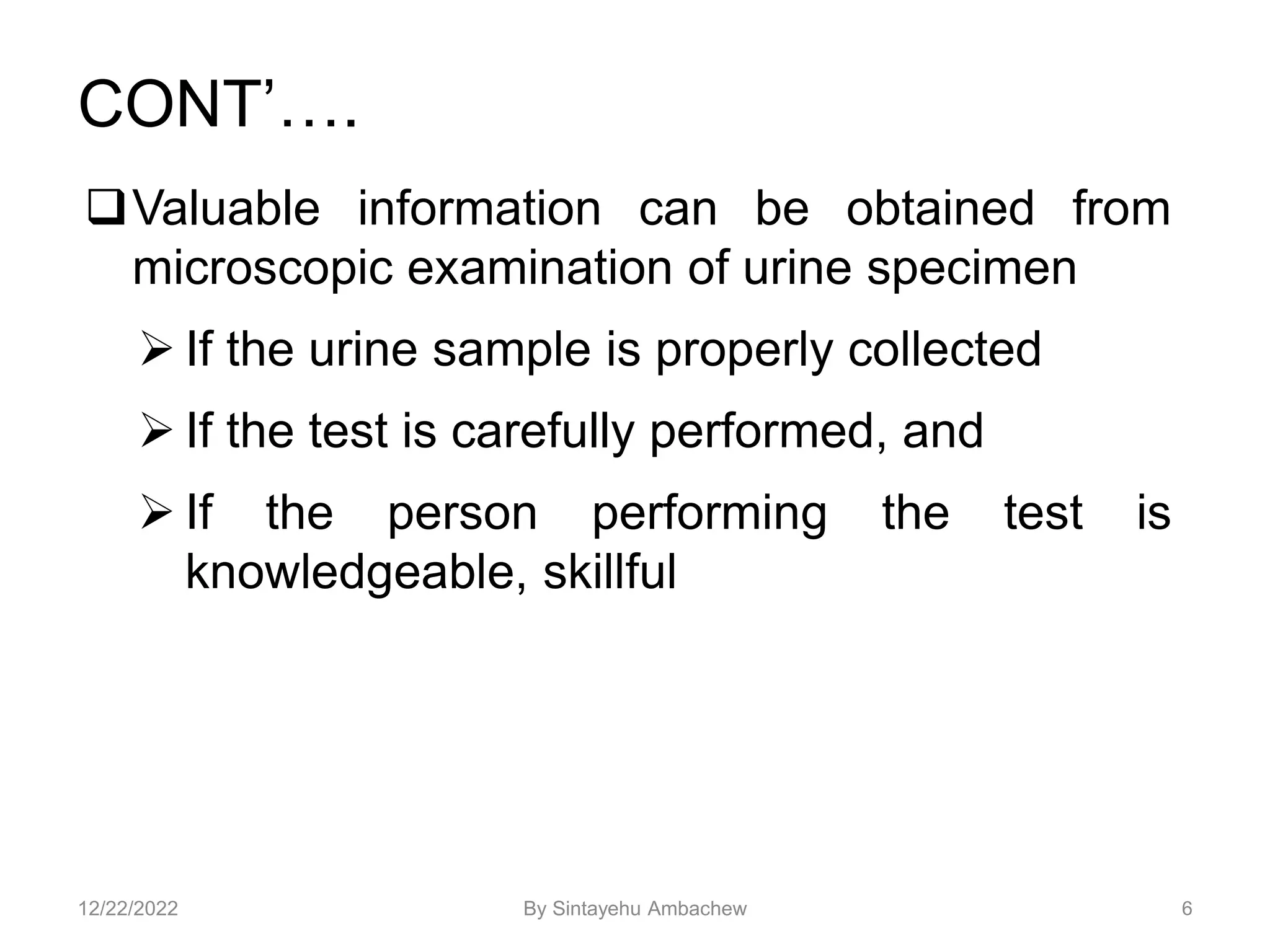
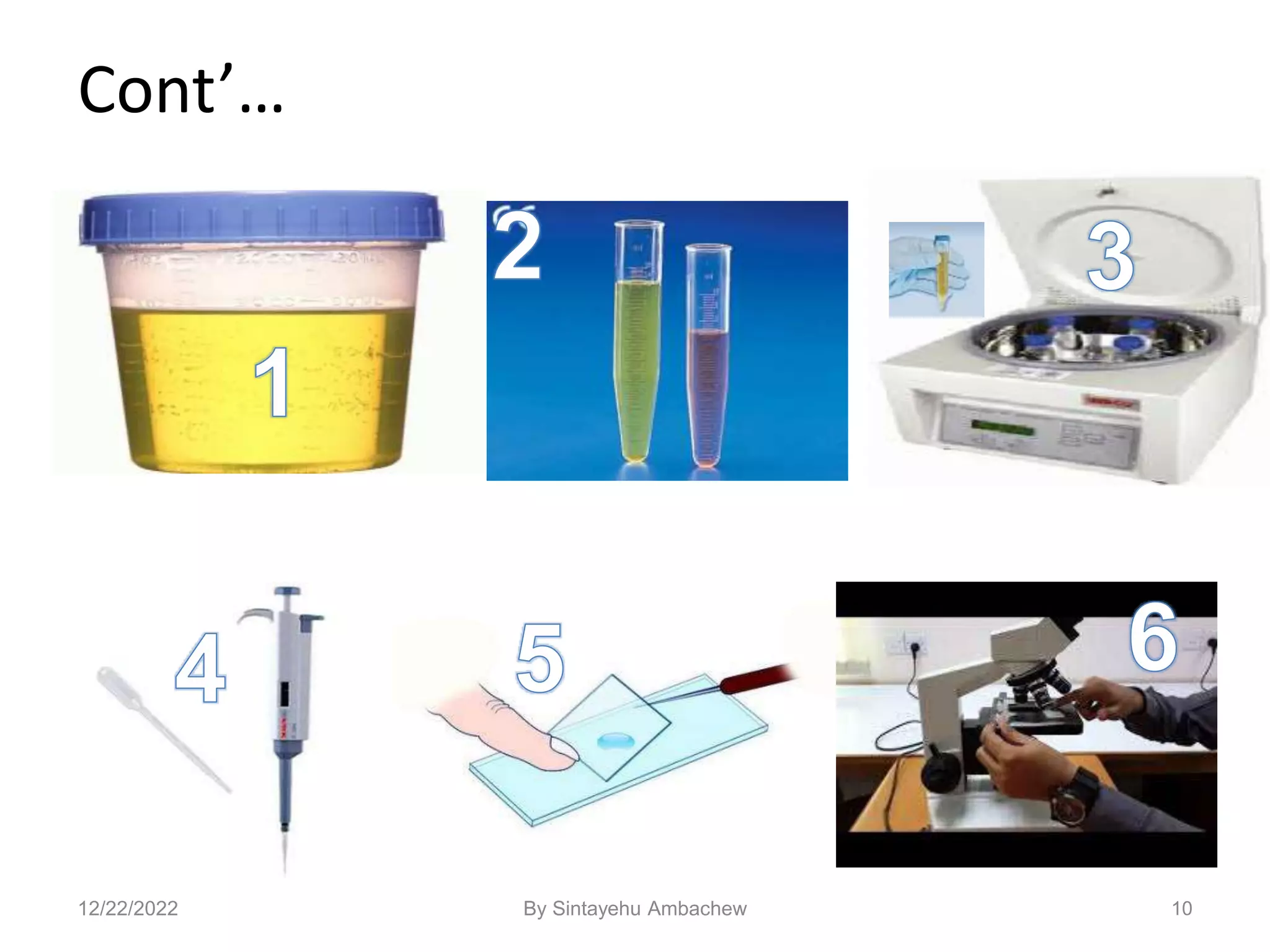
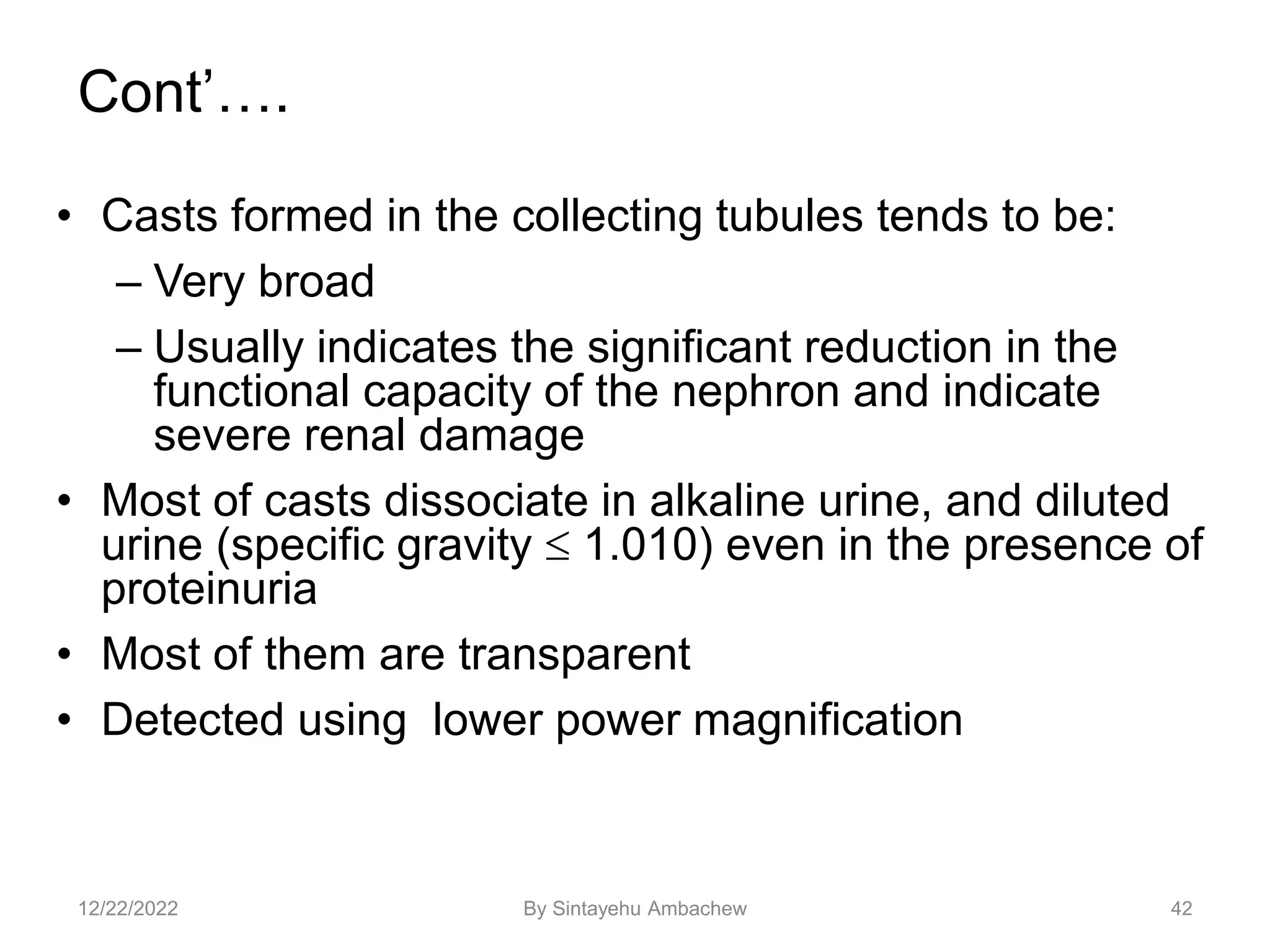
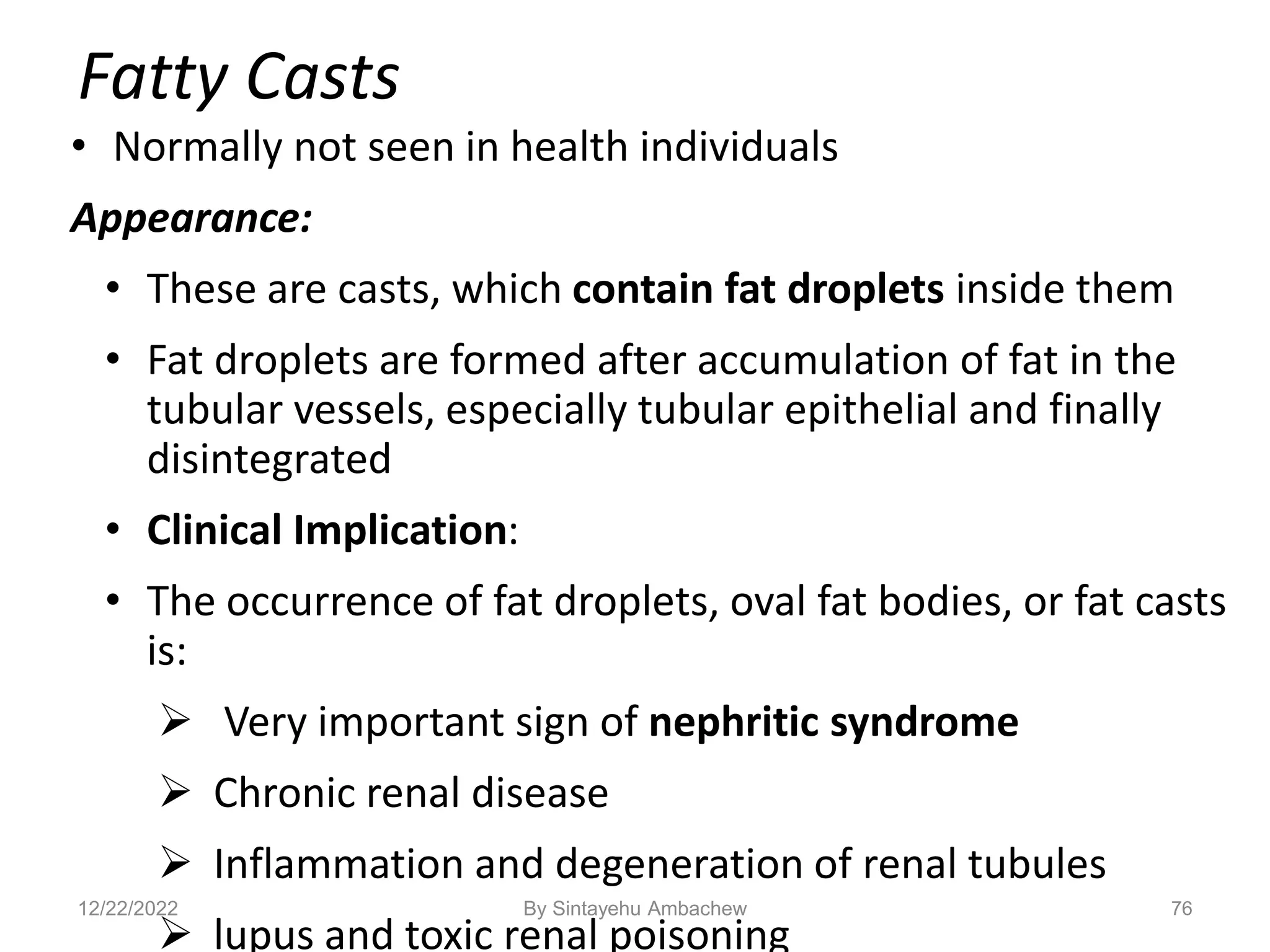
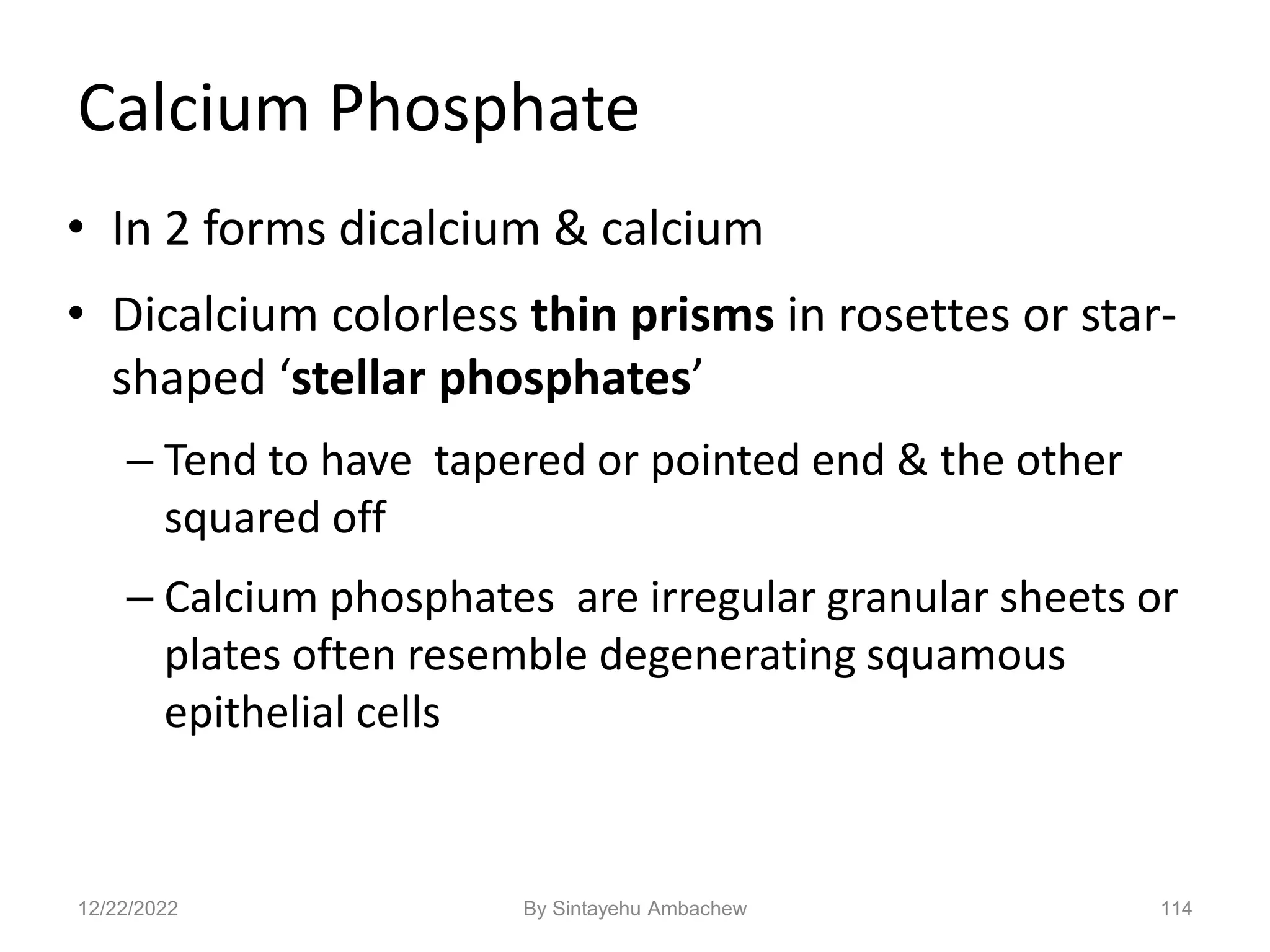
Amino Acid Crystals
• Tyrosine
– fine, delicate needles,
colorless or yellow
– frequently in clusters or
sheaves [as in stacks of
wheat]
– seen singly or in small
groups
– in acidic urine
– less soluble than leucine, so
found more often
12/22/2022 By Sintayehu Ambachew](https://image.slidesharecdn.com/microscopicexaminationofurinesediments-221222023650-c3614b1d/75/Microscopic-examination-of-Urine-sediments-ppt-121-2048.jpg)
![123
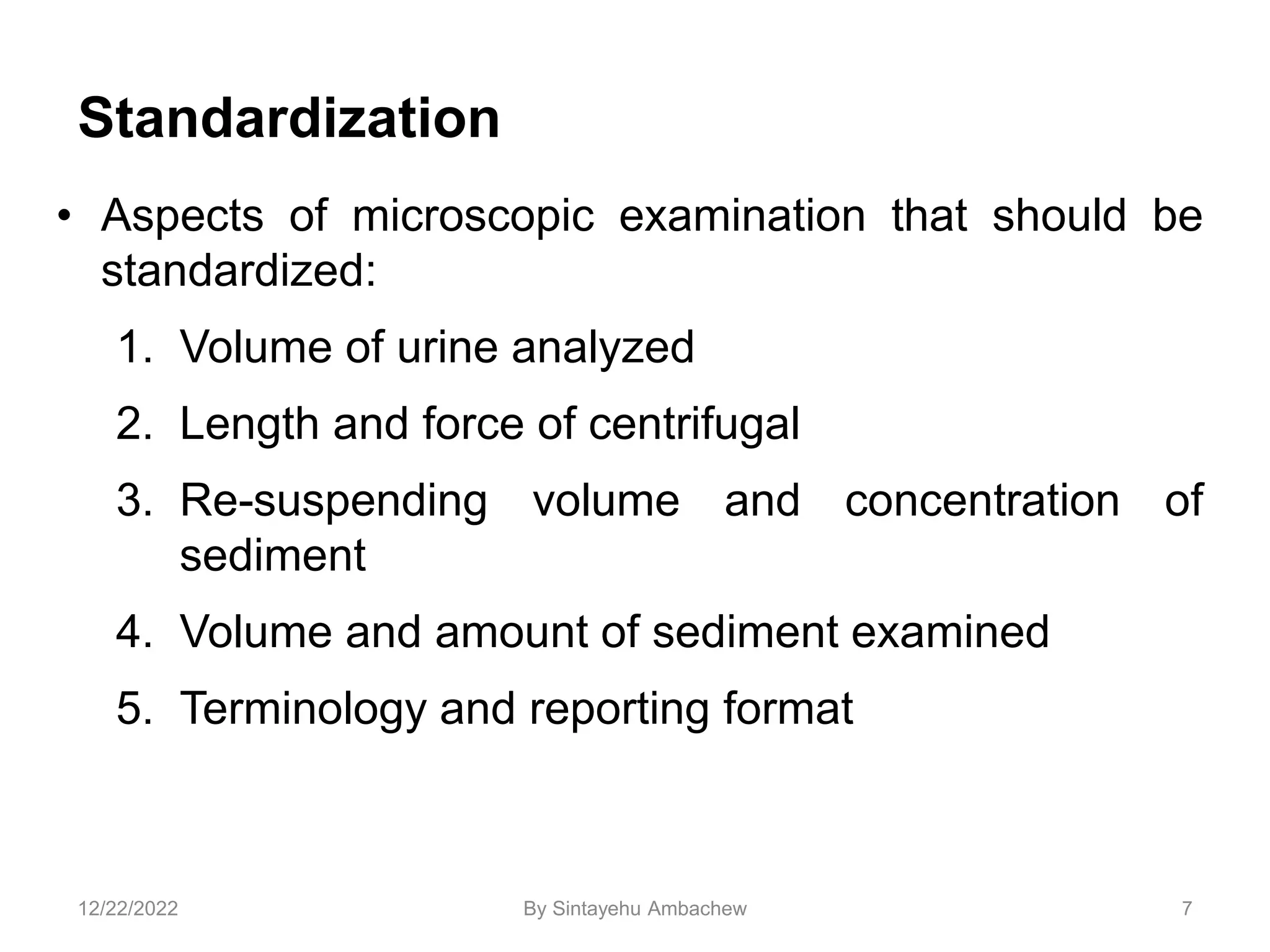
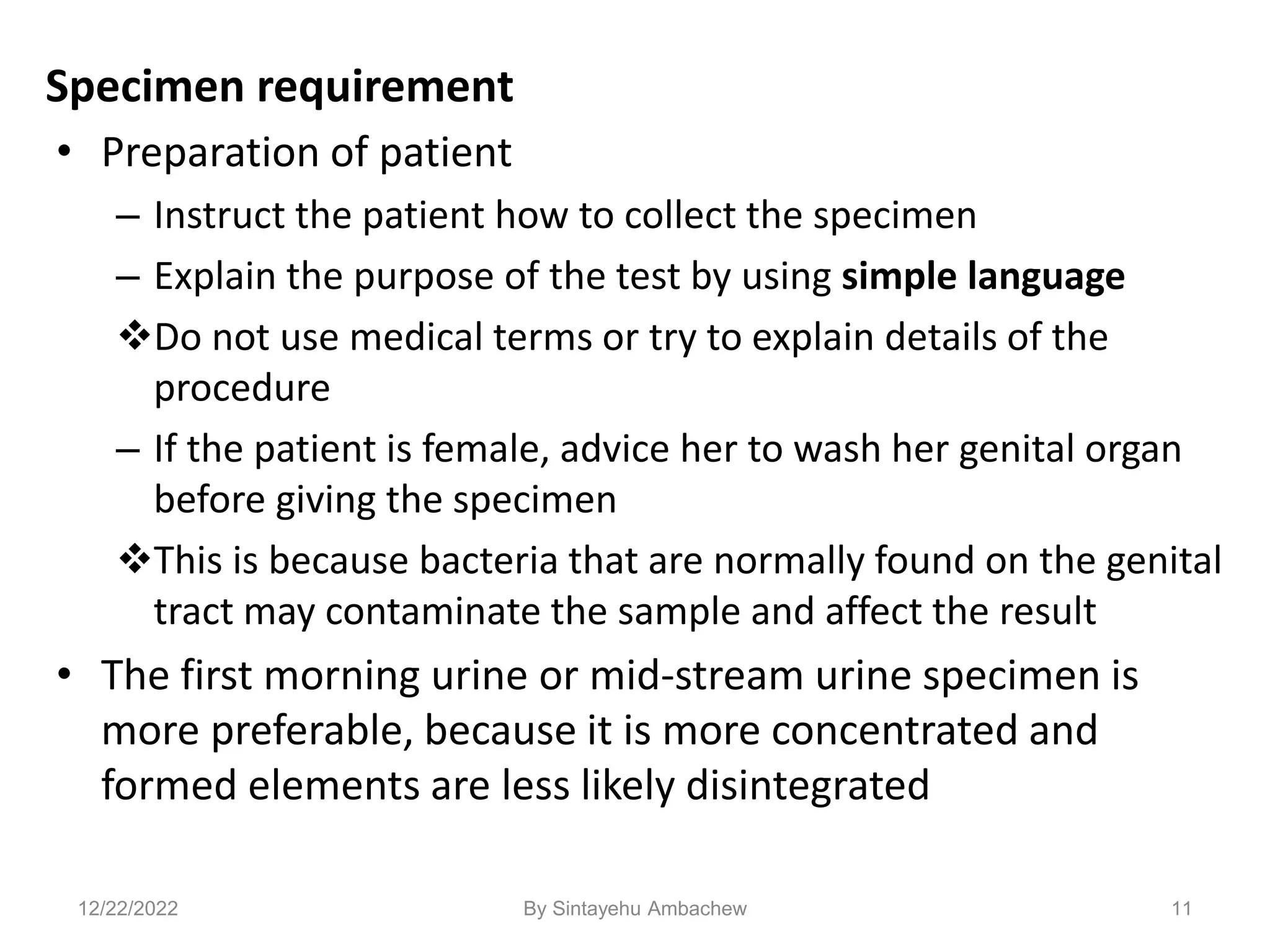
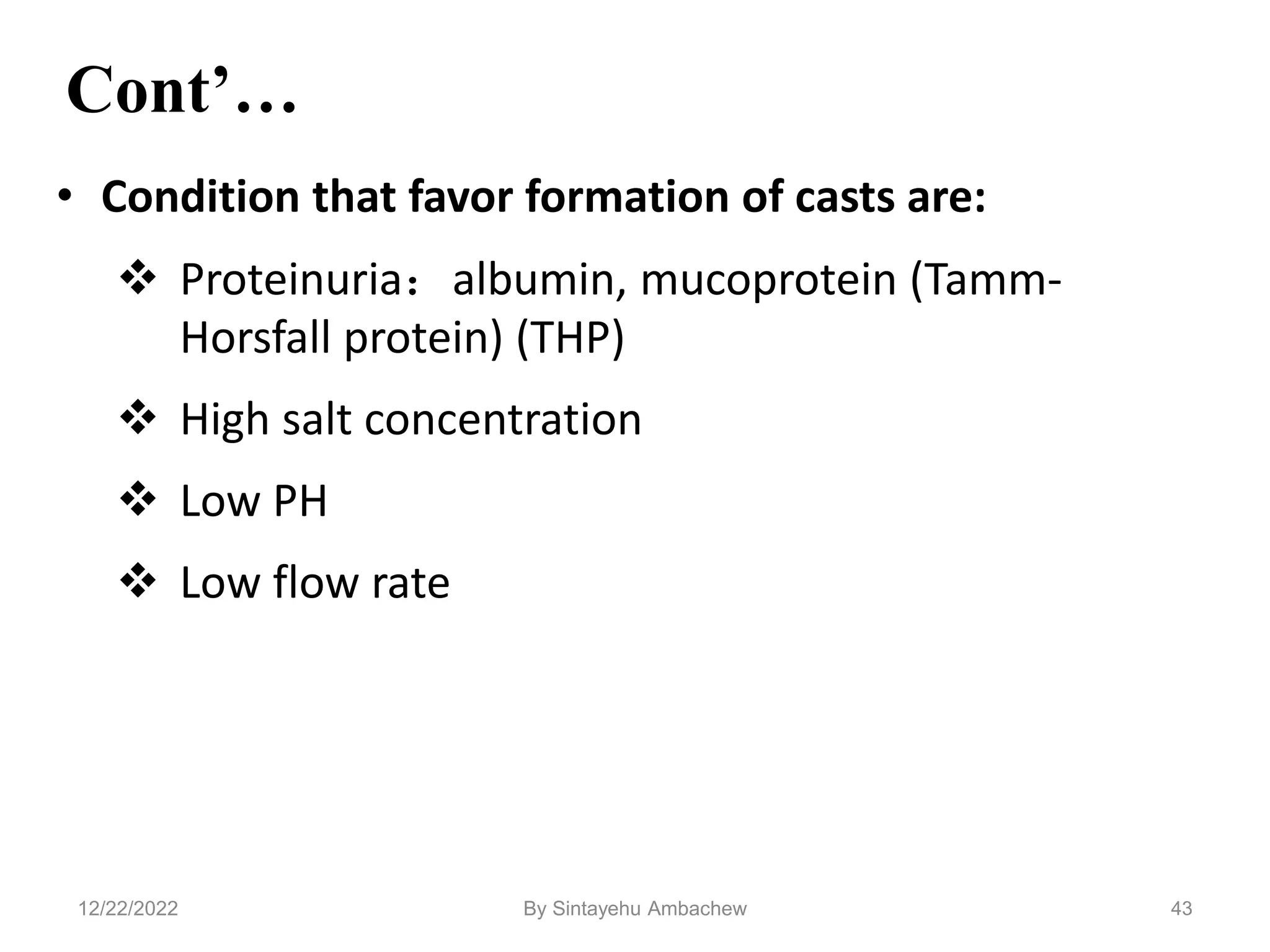
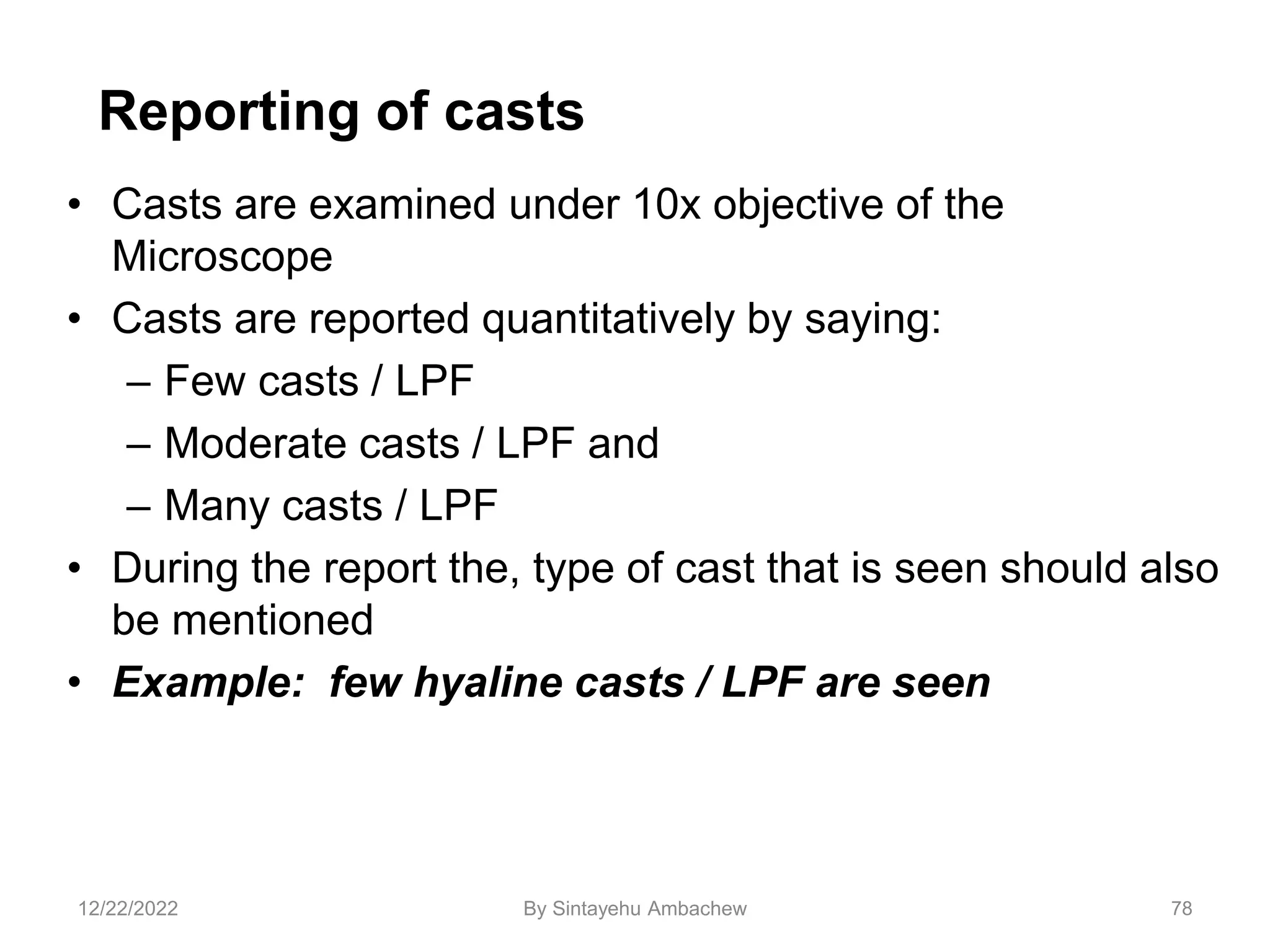
Leucine
• Highly refractile yellow to brown
spheres in acid urine.
• Have concentric/radial striations
on their surface
• Can be mistaken for fat globules
[or vice versa]
• But will not stain with fat stains
or appear as maltese cross under
polarization
• Can be seen in urine containing
tyrosine crystals if use alcohol to
‘precipitate’ Bactrim has similar appearance
check patient history
12/22/2022 By Sintayehu Ambachew](https://image.slidesharecdn.com/microscopicexaminationofurinesediments-221222023650-c3614b1d/75/Microscopic-examination-of-Urine-sediments-ppt-122-2048.jpg)
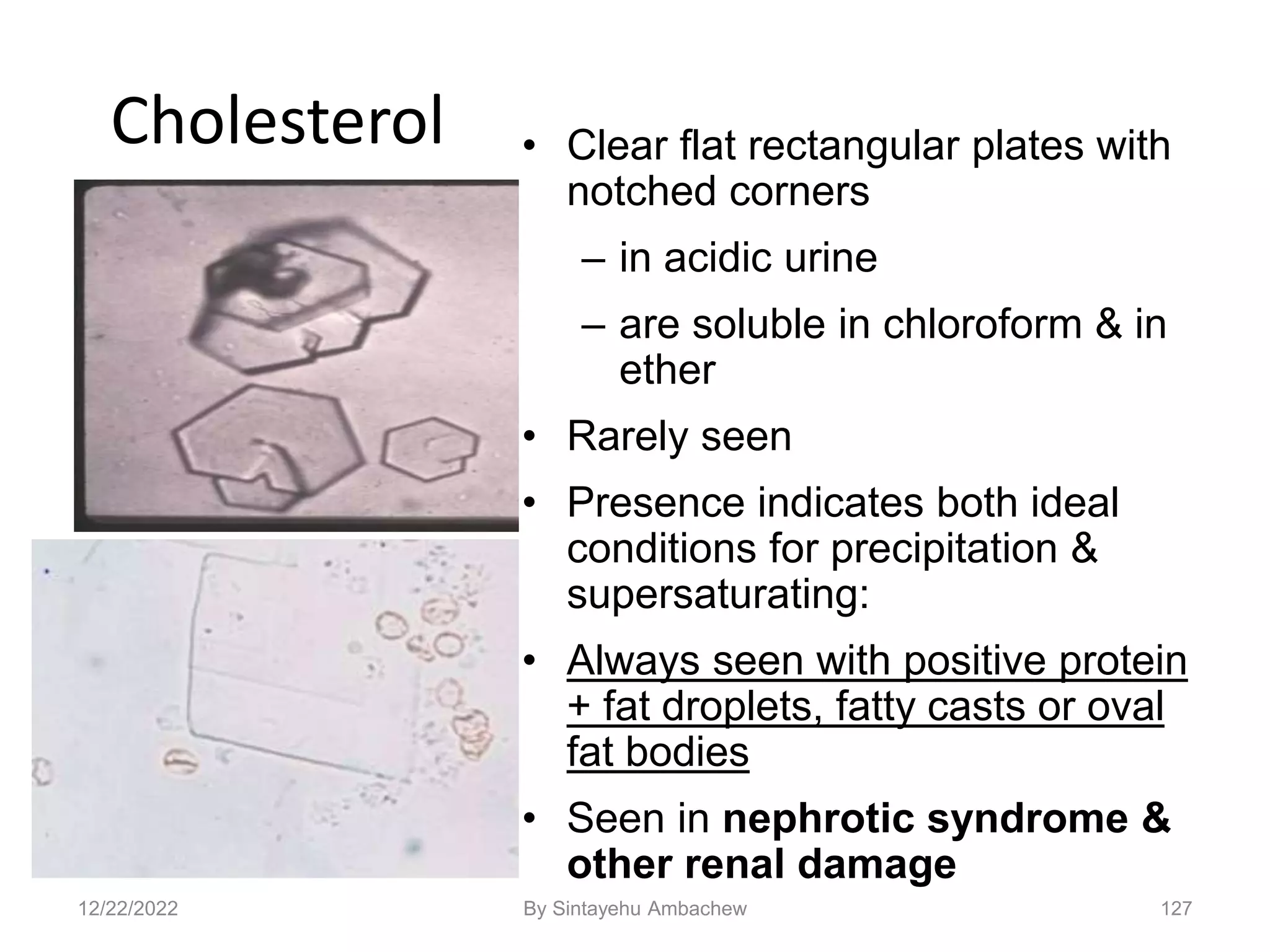
![128
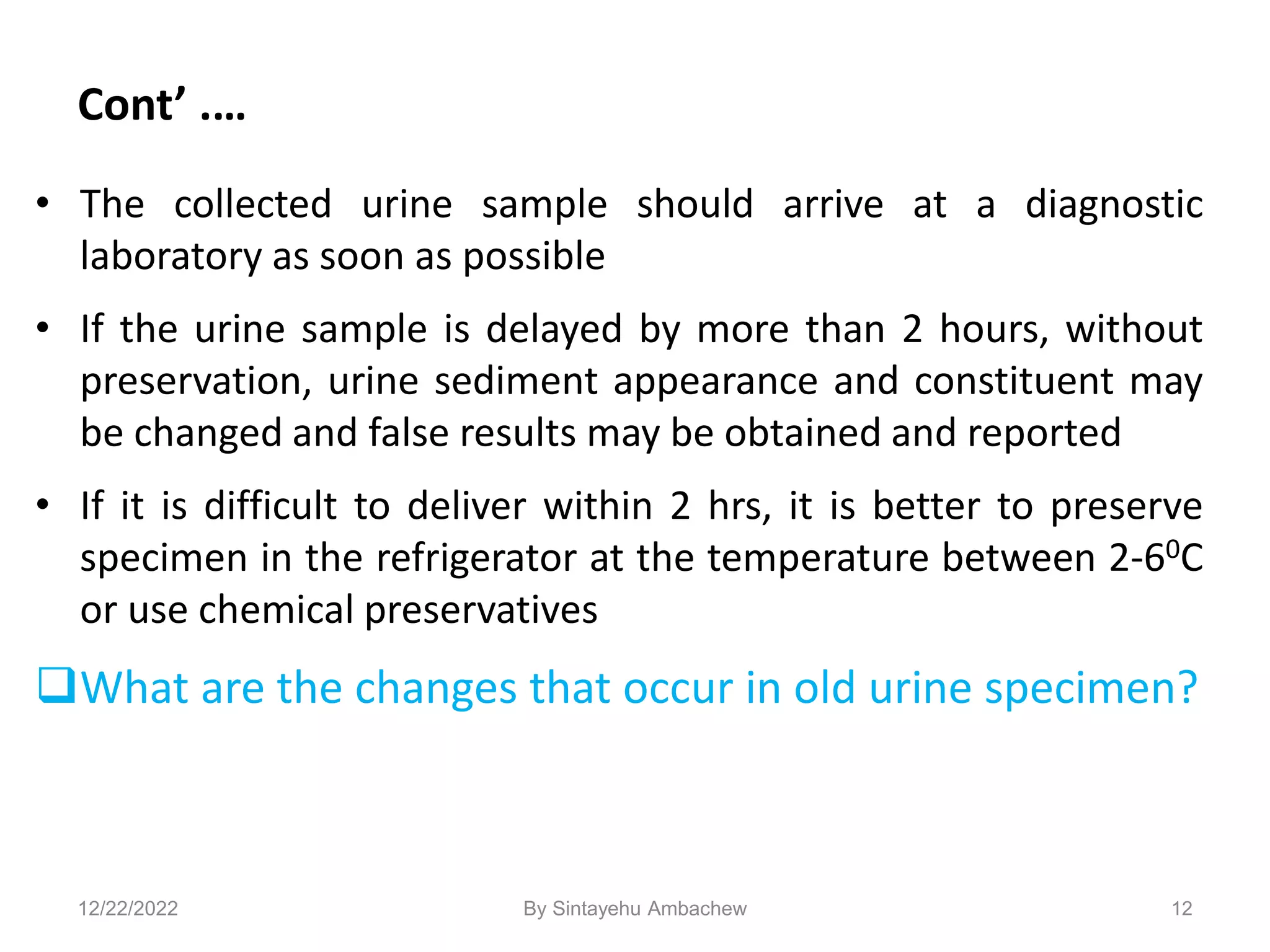
Confounding Conditions
• Radiopaque contrast medium [diatrizoate meglumine ] can be
mistaken for cholesterol
– Contrast medium will give abnormally high S.G. >1.040
– Not associated with proteinuria or lipiduria
– Cholesterol crystals found with normal S.G.
• Medications
– Can be excreted in high concentrations, resulting in precipitation
– These crystals are termed ‘iatrogenic’
– Proper identification of drug crystals important in alerting to
potential renal tubular damage
12/22/2022 By Sintayehu Ambachew](https://image.slidesharecdn.com/microscopicexaminationofurinesediments-221222023650-c3614b1d/75/Microscopic-examination-of-Urine-sediments-ppt-127-2048.jpg)


























![Cytopathology Of Cerebrospinal Fluid[1]Power Point](https://cdn.slidesharecdn.com/ss_thumbnails/cytopathologyofcerebrospinalfluid1power-point-1230479978520994-2-thumbnail.jpg?width=640&height=640&fit=bounds)





























![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)











