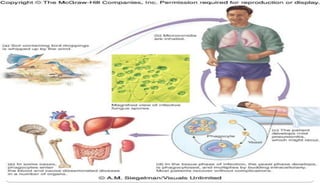
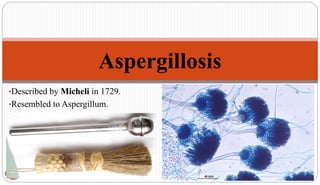
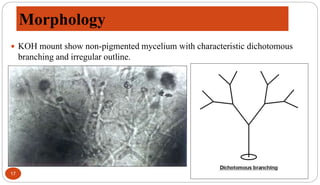
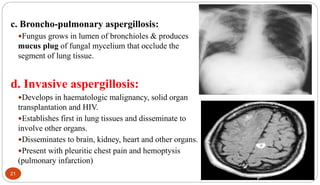
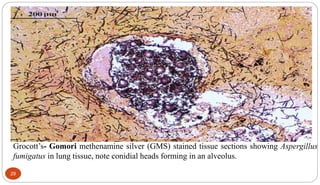
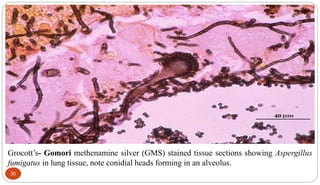
Fungal Pneumonia can be caused by several fungi including Histoplasma capsulatum, Aspergillus fumigatus, Candida albicans, Coccidioides immitis, and Pneumocystis jirovecii. Histoplasmosis, caused by Histoplasma capsulatum, is one of the most common fungal infections worldwide. It typically presents as an acute pulmonary infection after exposure to bird or bat droppings but can become chronic or disseminate without treatment. Aspergillosis, caused by Aspergillus fumigatus, is an opportunistic infection seen in immunocompromised individuals. It ranges from allergic forms to invasive pneumonia