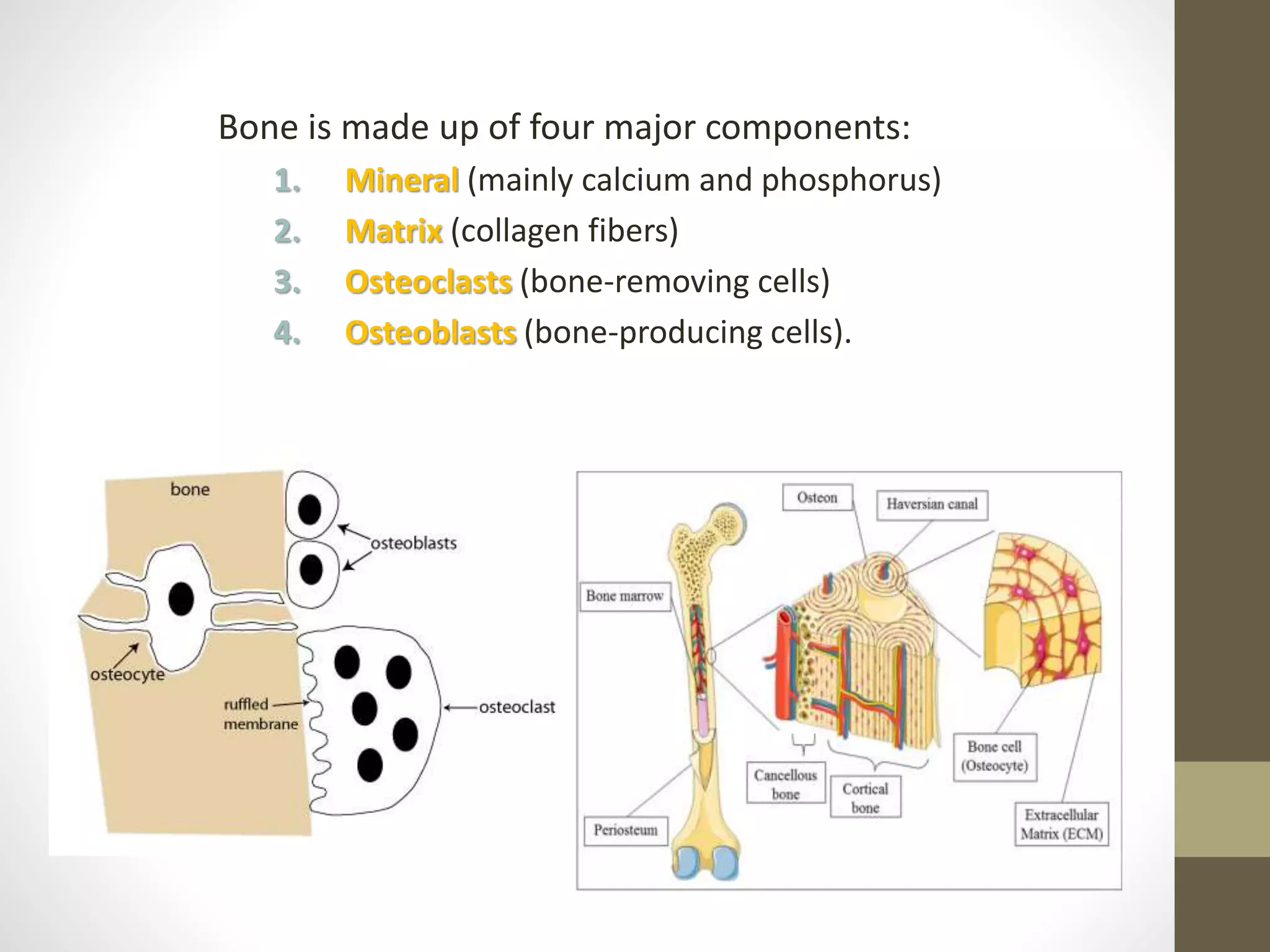
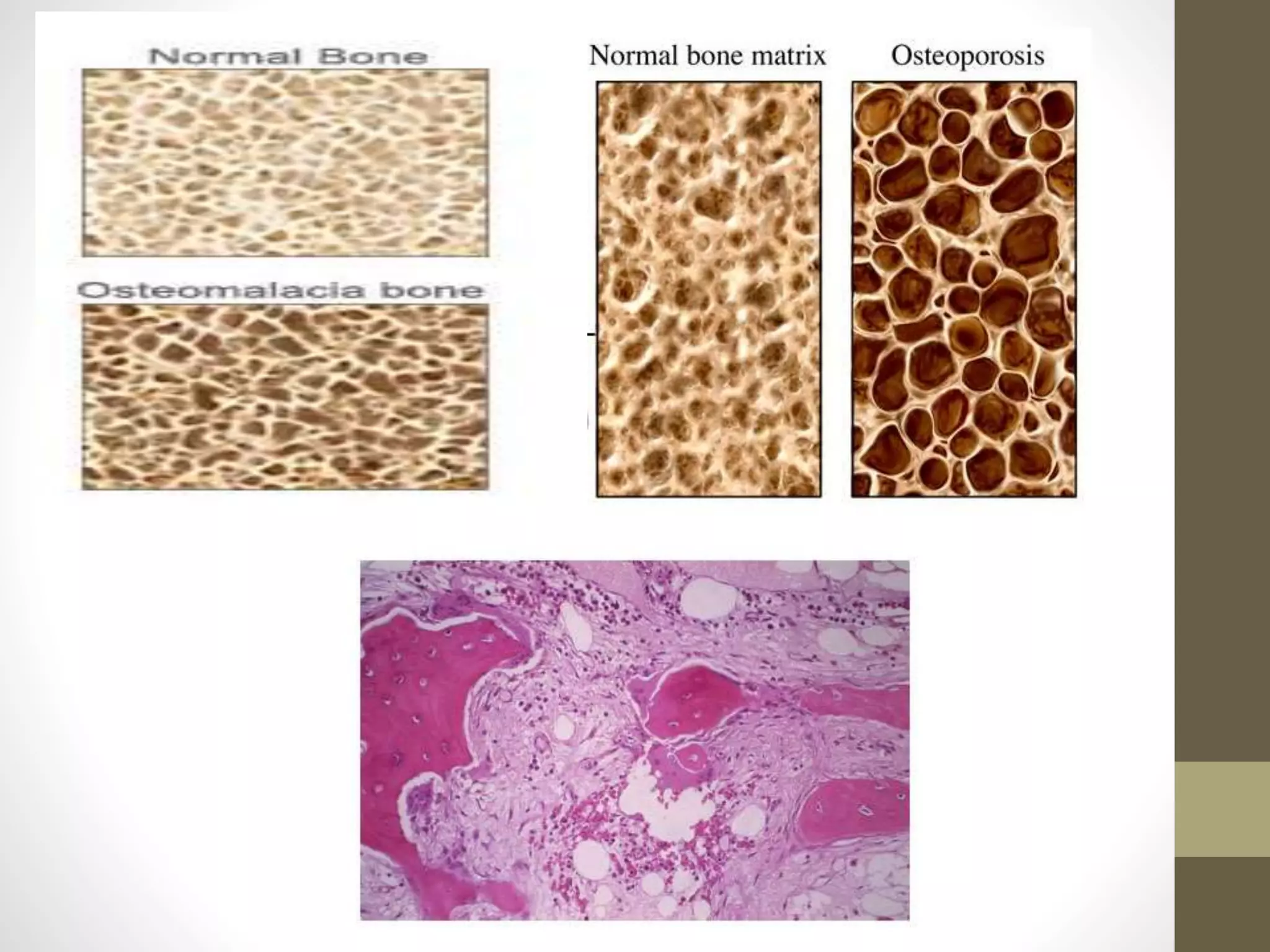
This document discusses metabolic bone diseases including osteoporosis, osteomalacia, and rickets. It describes the components of bone, common metabolic bone disorders, clinical assessment, x-ray findings, bone density measurement techniques, biochemical tests, and treatment approaches for various conditions like postmenopausal osteoporosis, vitamin D deficiency rickets, hypophosphatemic rickets, and osteomalacia in adults.