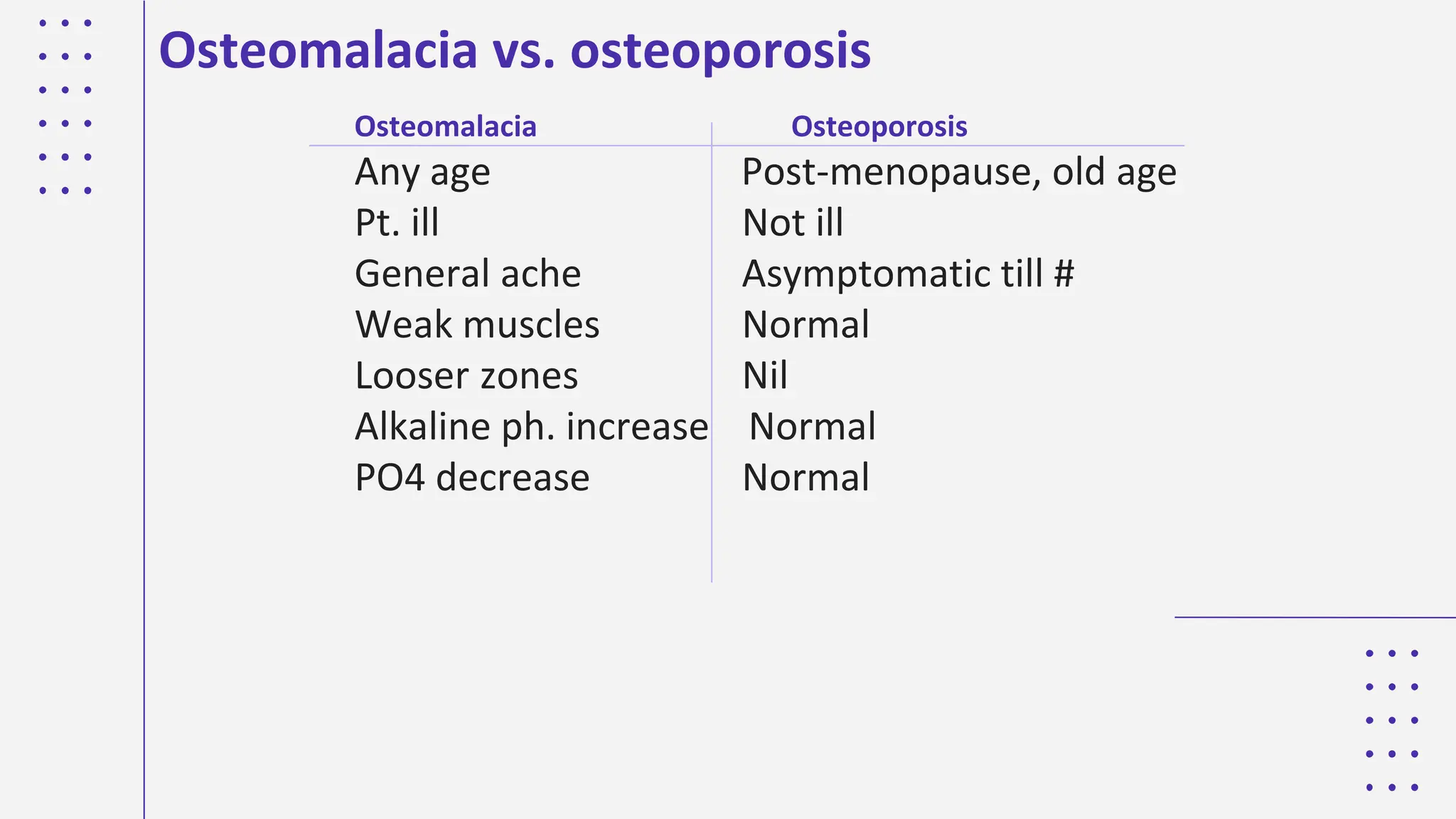
The document covers various metabolic bone diseases, focusing on their classification, imaging techniques, and management strategies. Key conditions discussed include osteoporosis, osteomalacia, rickets, hyperparathyroidism, renal osteodystrophy, and Paget's disease, along with their effects on bone structure and function. It concludes with the importance of understanding these diseases for accurate diagnosis and treatment in radiology.