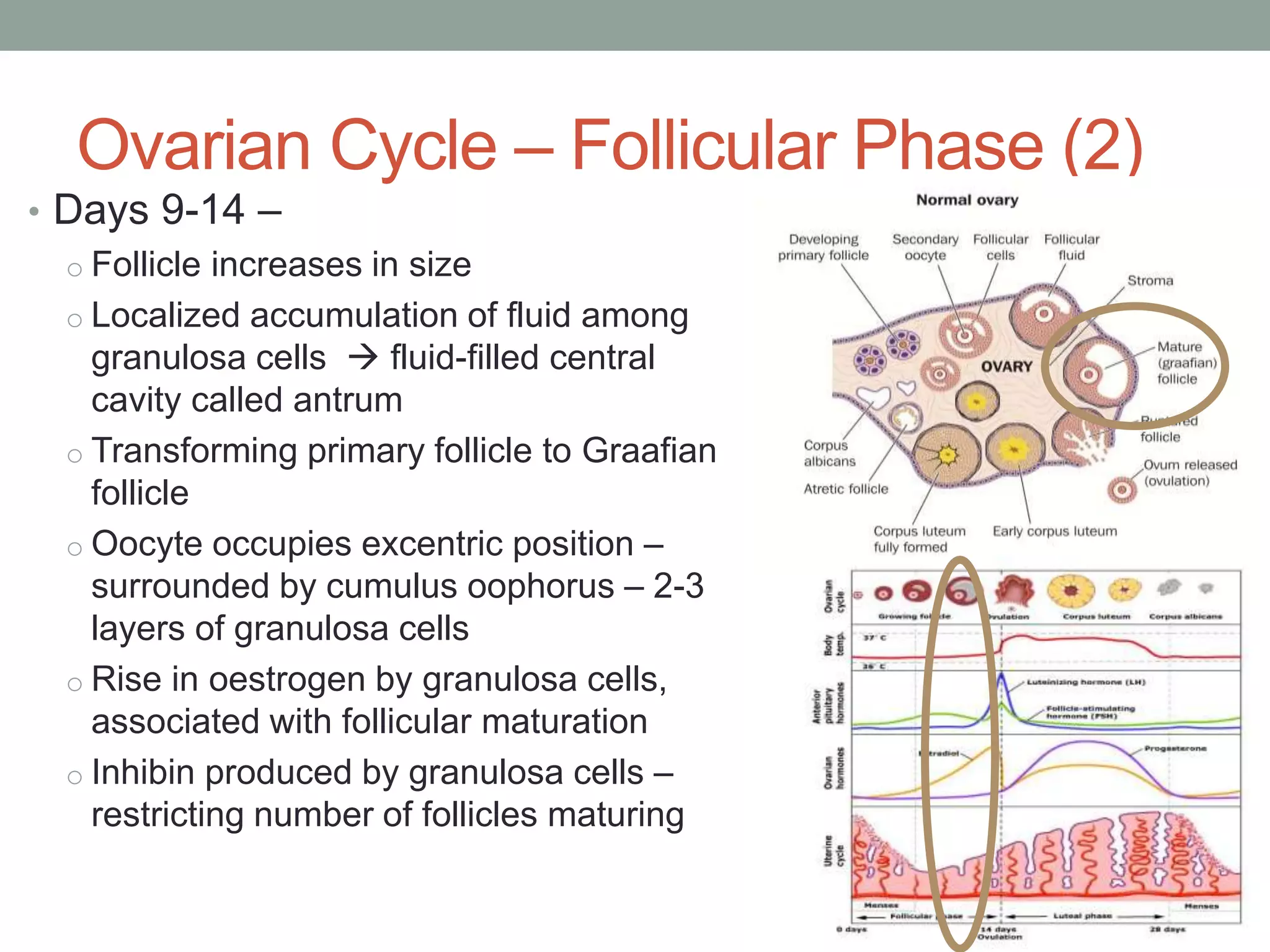
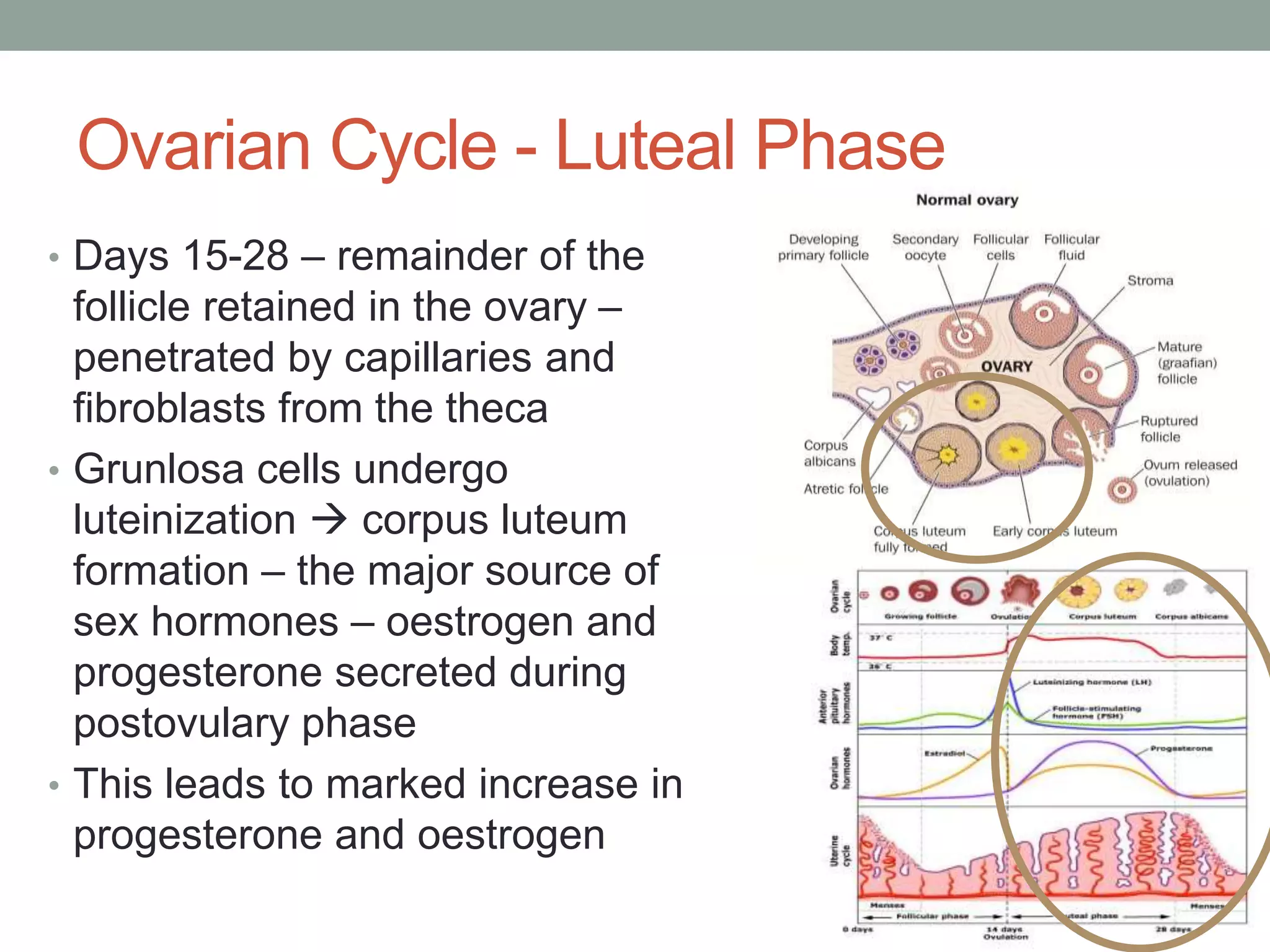
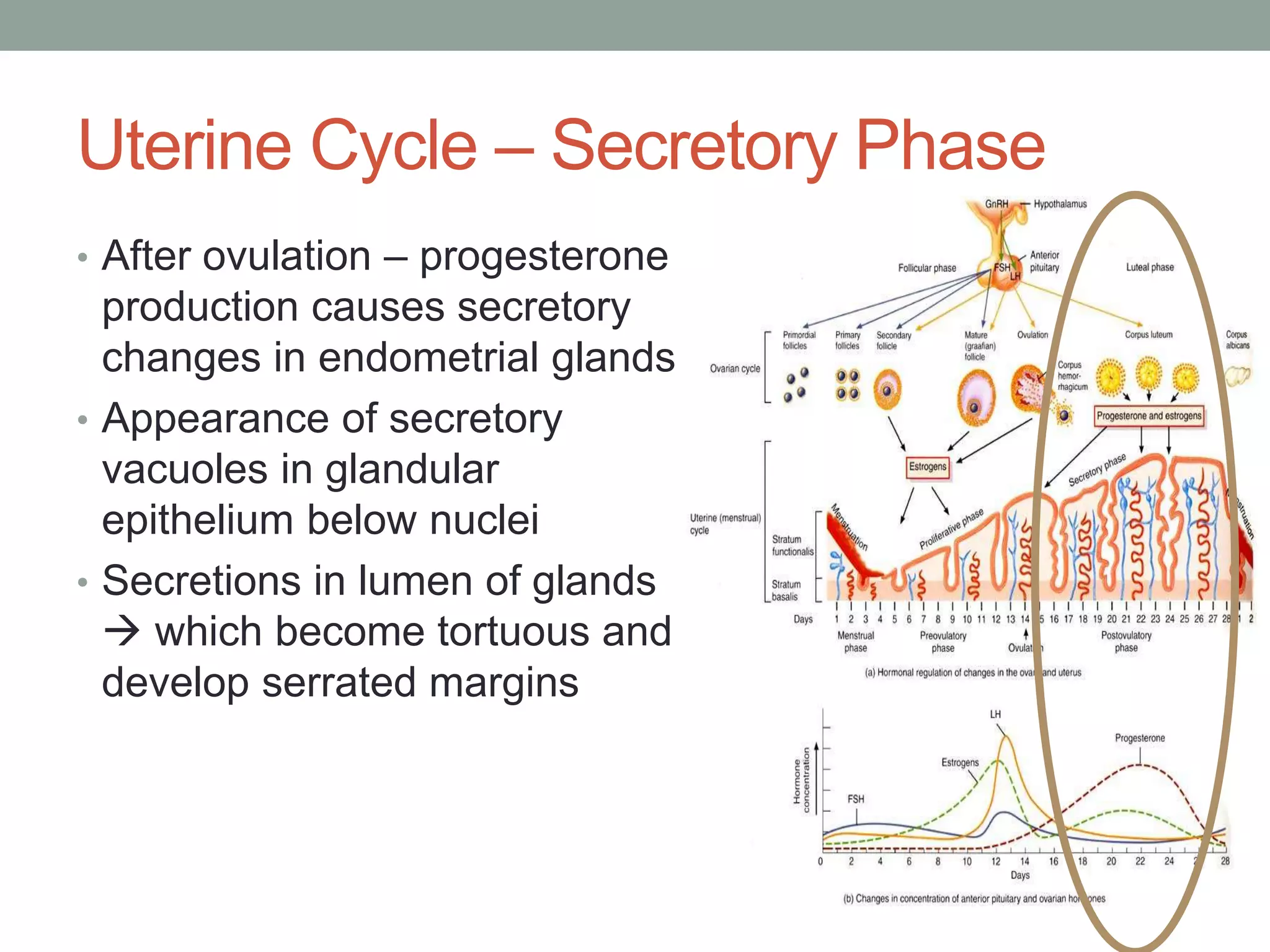
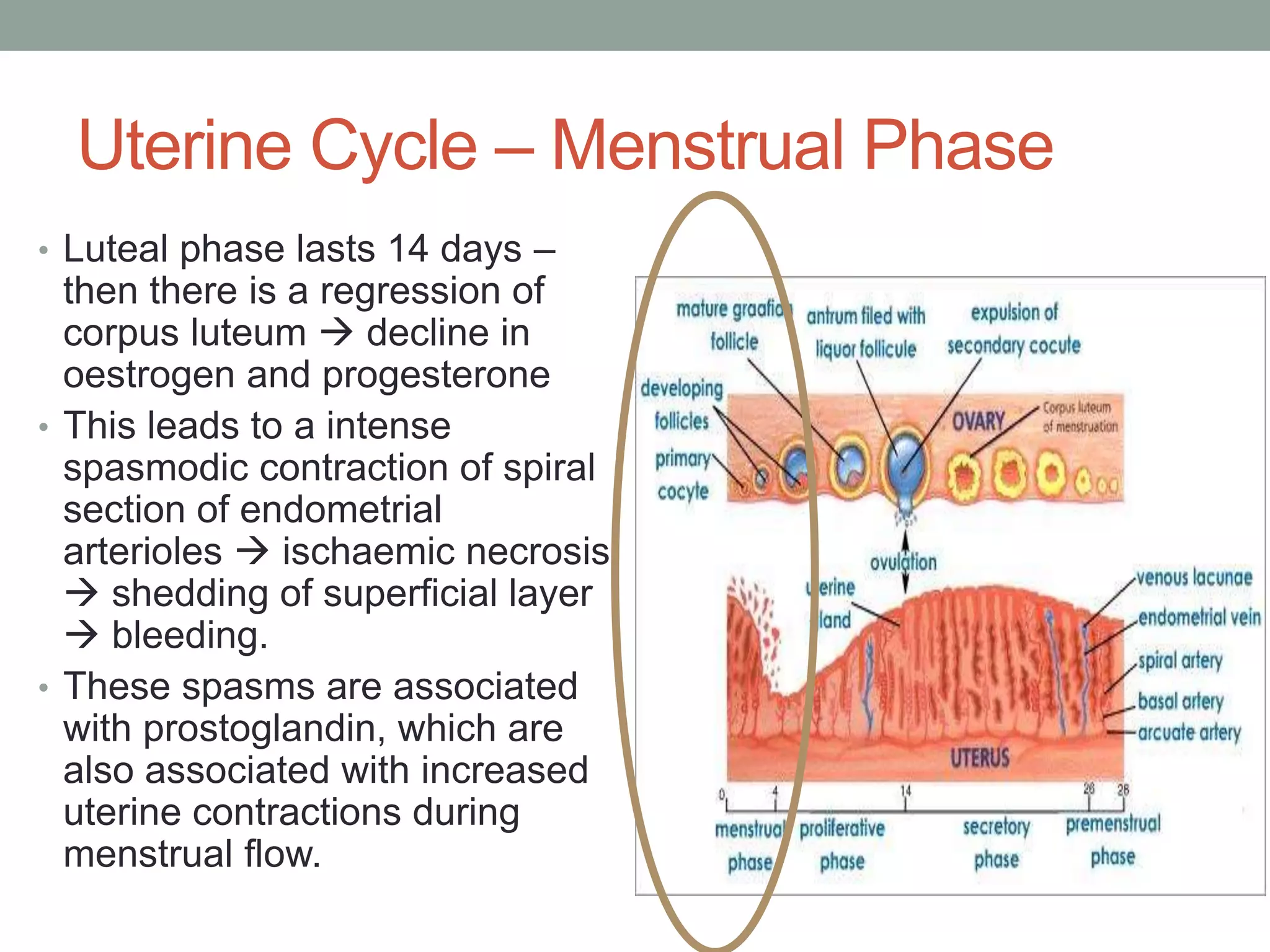
The menstrual cycle involves coordinated changes in the ovaries and uterus driven by hormones. It typically lasts 28 days and includes a follicular phase where an egg matures and is released, ovulation, and a luteal phase where the corpus luteum develops. Hormones like FSH, LH, estrogen and progesterone regulate this cycle. The endometrium thickens during the follicular phase in response to rising estrogen, and further changes during the luteal phase due to progesterone to prepare for potential implantation. If implantation does not occur, hormone levels drop and the endometrium is shed as menstruation.