Downloaded 83 times
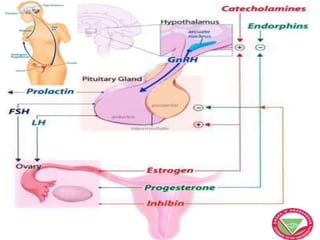

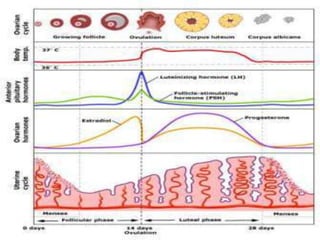

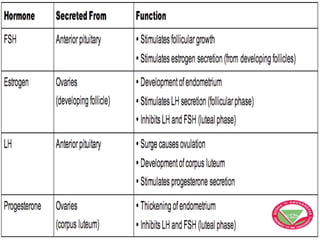
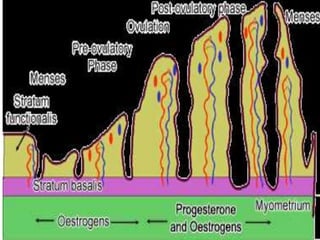


The menstrual cycle describes the monthly changes women's bodies go through from the start of menstruation to ovulation and then back to menstruation. It involves both ovarian and uterine cycles controlled by hormones. The ovarian cycle consists of the follicular phase where an egg develops and is released at ovulation, and the luteal phase where the corpus luteum forms. The uterine cycle involves changes to the endometrium driven by hormones, from proliferation to secretion to menstruation. Key events include the development and rupture of the ovarian follicle, formation and regression of the corpus luteum, and shedding of the uterine lining if implantation does not occur.














































































