This document discusses malnutrition and nutritional support. Some key points:
- 30-60% of surgical and hospitalized patients are malnourished, increasing risks of complications and death.
- Malnutrition causes metabolic changes like increased protein catabolism and reduced energy expenditure. Trauma/sepsis increases requirements and causes insulin resistance.
- Nutritional assessment tools include BMI, weight loss percentage, albumin levels, and MUST screening tool.
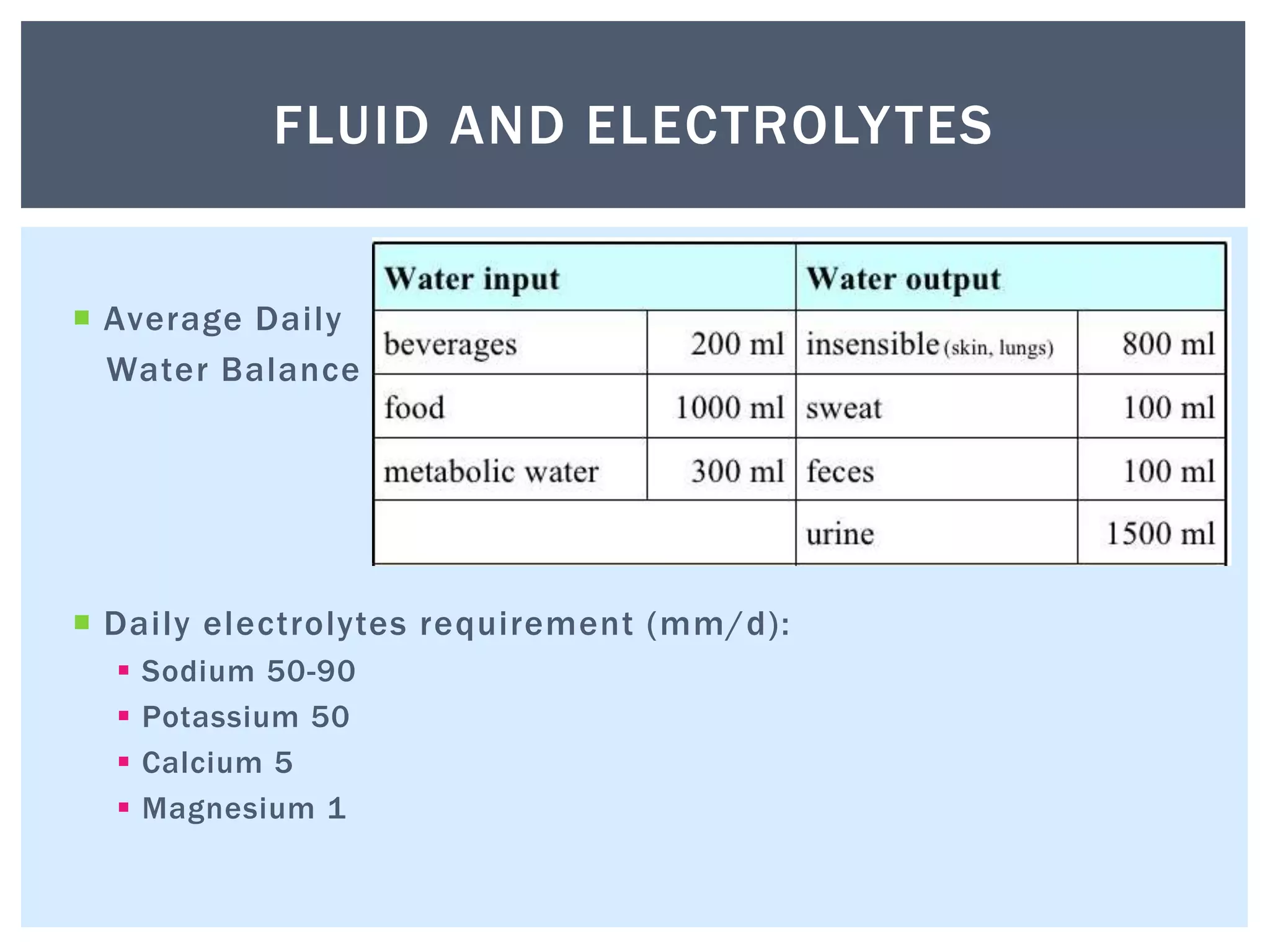
- Fluid requirements are based on condition and losses. Common IV fluids include Hartmann's, normal saline, dextrose saline, and colloids. Electrolytes like sodium and potassium are also essential.
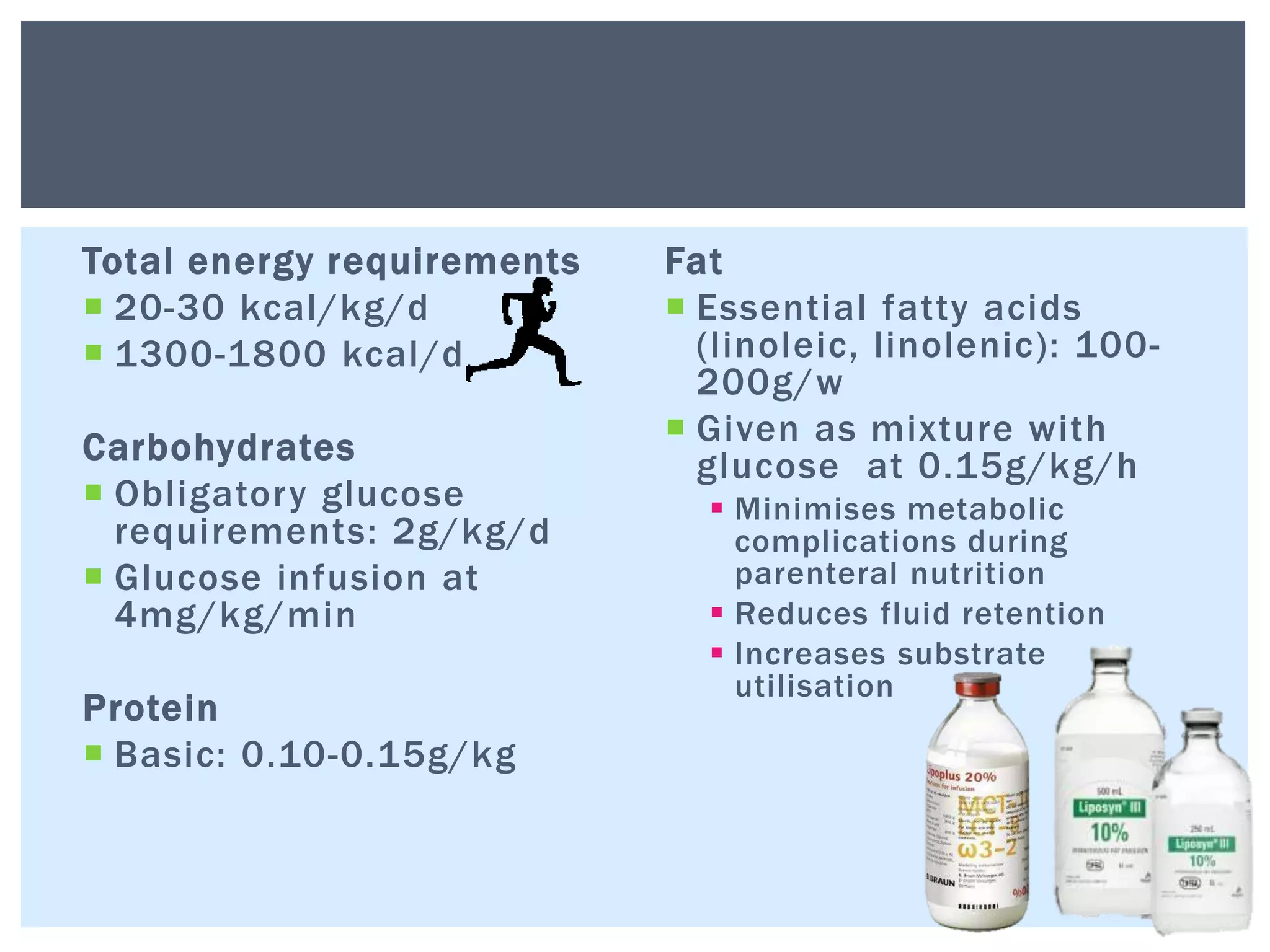
- Nutritional support aims to meet caloric, protein