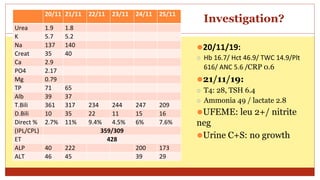
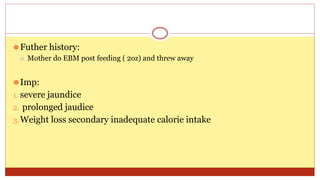
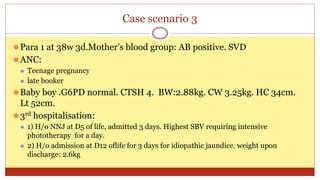
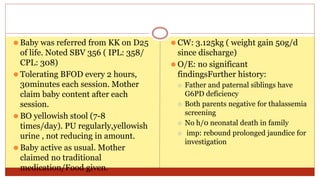
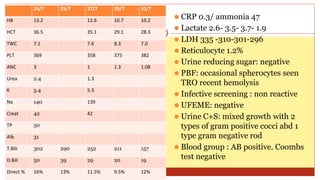
- This document presents 3 case scenarios of neonatal jaundice. The first case involves a 2-day old female infant with a serum bilirubin of 272 referred for poor breastfeeding and phototherapy. The second case involves a 10-day old male infant referred for jaundice and weight loss with a bilirubin of 310. The third case involves a 25-day old male infant with a history of jaundice and admissions with a current bilirubin of 356.
























































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
