Downloaded 795 times


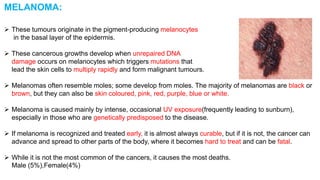
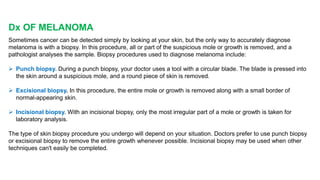

Melanoma is a type of skin cancer that develops from pigment-producing cells known as melanocytes. It is caused by unrepaired DNA damage and mutations in these cells that lead to uncontrolled growth. While not the most common cancer, melanoma is particularly dangerous due to its ability to spread quickly if not detected early. Risk factors include excessive sun exposure, the presence of many moles or abnormal moles, fair skin, and family history. There are different types of melanoma that can vary in appearance, location, and growth patterns. Early detection of melanoma greatly increases survival rates.


































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
















