Downloaded 234 times



![PHYSICAL EXAMINATION:
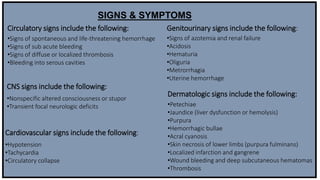
• Look for symptoms and signs of thrombosis in large vessels (eg, [DVT]) and microvascular thrombosis (as in
renal failure).
• Bleeding from at least 3 unrelated sites is particularly suggestive of DIC. As many as 25% of patients present
with renal failure.
• Patients with pulmonary involvement can present with dyspnoea, haemoptysis, and cough. Comorbid liver
disease as well as rapid haemolytic bilirubin production may lead to jaundice.
• Neurologic changes (eg, coma, altered mental status, and paraesthesia) are also possible.
With acute DIC, the physical findings are usually those of the underlying or inciting condition; however, patients
with the acute disease (i.e., the haemorrhagic variety associated with excess plasmin formation) have Petechiae on
the soft palate, trunk, and extremities from thrombocytopenia and ecchymosis at venepuncture sites. These
patients also manifest ecchymosis in traumatized areas.
In patients with so-called chronic or sub acute DIC, of which the primary manifestation is thrombosis from excess
thrombin formation, the signs of venous thromboembolism may be present.](https://image.slidesharecdn.com/dicsyndrome-150202053224-conversion-gate01/85/Dic-syndrome-6-320.jpg)

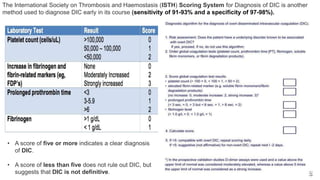





Disseminated intravascular coagulation (DIC) is an acquired syndrome where there is widespread activation of the coagulation system, leading to microvascular thrombosis and organ damage. It can occur acutely when large amounts of procoagulants are suddenly released, or chronically with small continuous releases over time. Left untreated, it can cause life-threatening hemorrhage. Diagnosis involves looking for signs of bleeding and thrombosis, as well as using scoring systems to assess coagulation markers. Treatment focuses on treating the underlying condition while providing supportive care and replacing clotting factors.