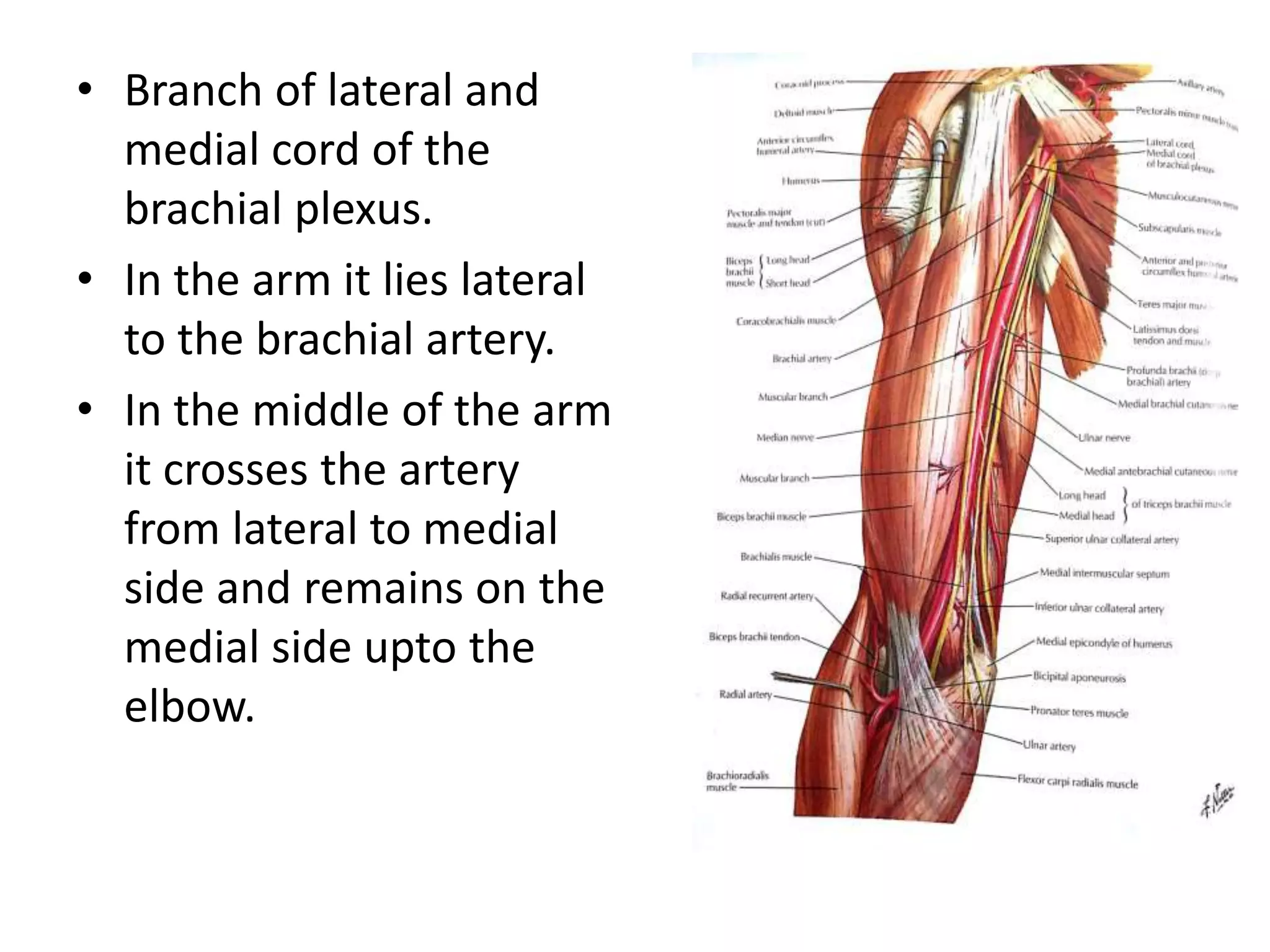
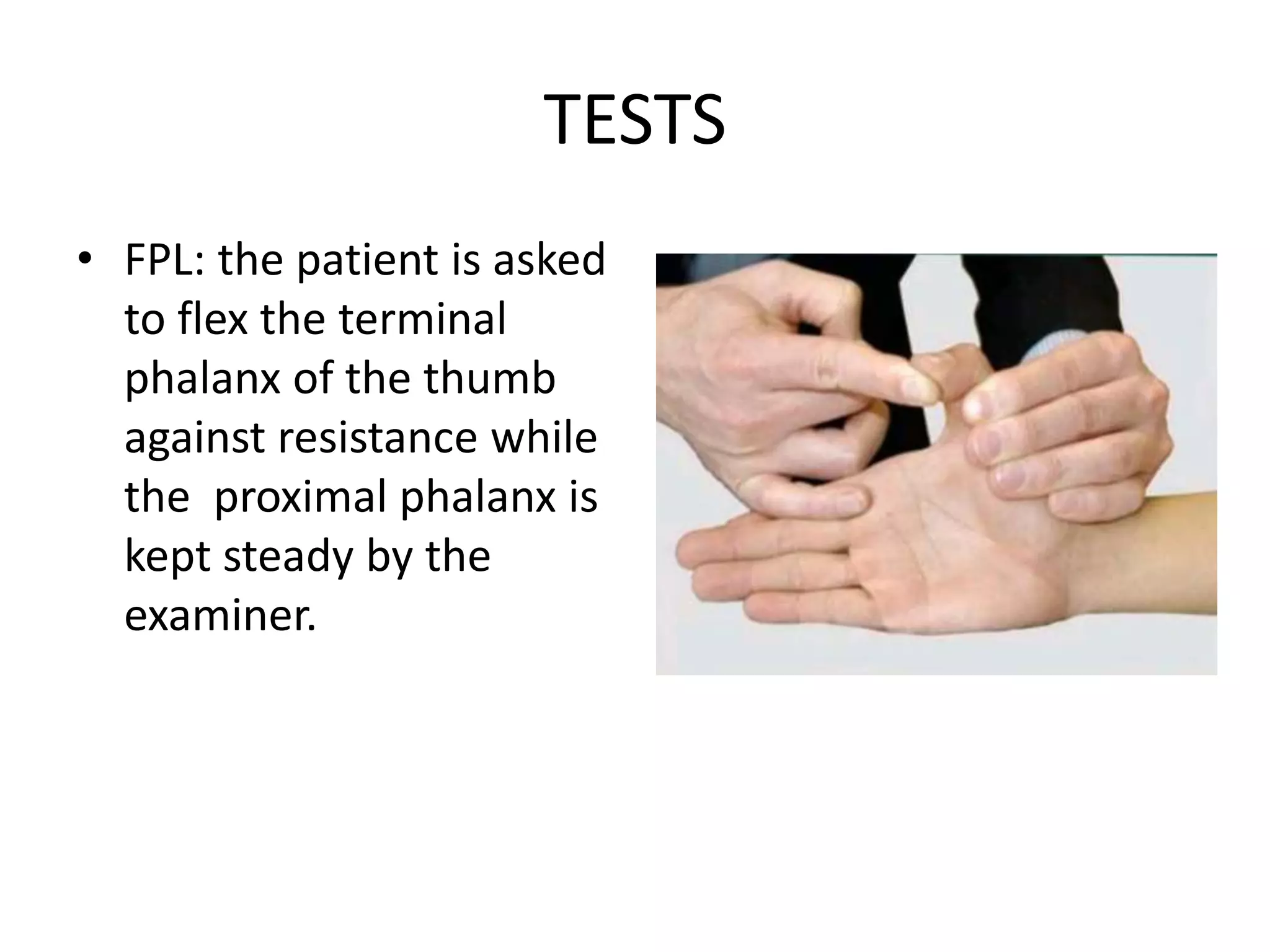
This document provides information on the median nerve including its course, branches, and clinical significance. It begins with the median nerve's origin from the brachial plexus and course through the arm. It then describes branches and distribution in the forearm, hand, and injuries such as carpal tunnel syndrome. Clinical tests for median nerve function and management options are also summarized.