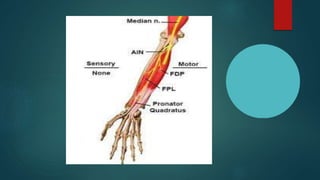
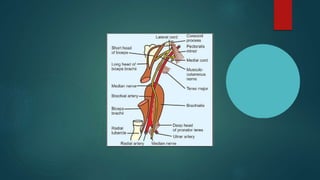
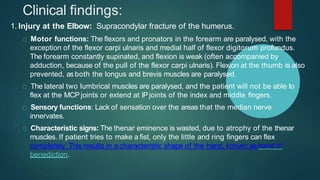
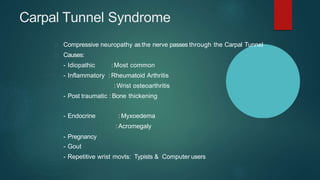
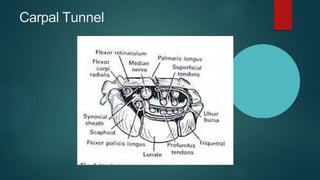
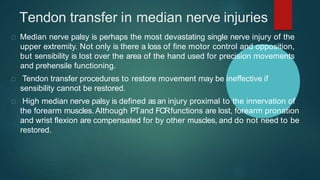
The median nerve provides both motor and sensory functions to parts of the forearm and hand. It innervates muscles that allow pronation of the forearm, flexion of the wrist, and flexion of the fingers. Sensory innervation is provided to the palmar surface and fingertips of the lateral three and a half digits. Median nerve injuries are commonly caused by fractures near the elbow or lacerations at the wrist. Carpal tunnel syndrome results from compression of the median nerve as it passes through the carpal tunnel in the wrist.













































![Peripheral Nerves of Upper Limb [Radial, Median & Ulnar nerve]](https://cdn.slidesharecdn.com/ss_thumbnails/sb-190709091558-thumbnail.jpg?width=640&height=640&fit=bounds)












































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)

















