

















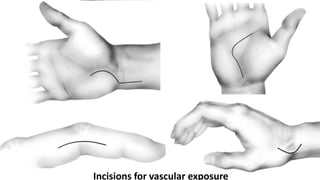


































The document provides an overview of hand anatomy including terminology, skin, fascia, muscles, tendons, bones, joints, nerves and vasculature. Key points include descriptions of various hand incisions and their purposes, fascial layers and spaces of the hand, flexor tendon anatomy and zones of injury, and anatomy of important muscles like the thenar and hypothenar muscles. The document covers the detailed functional anatomy of the hand.