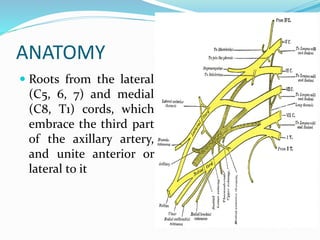
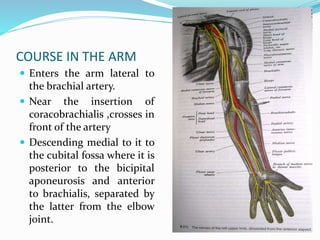
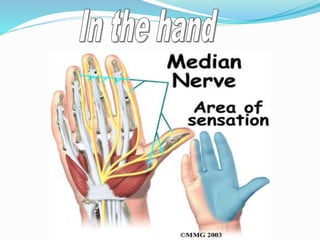
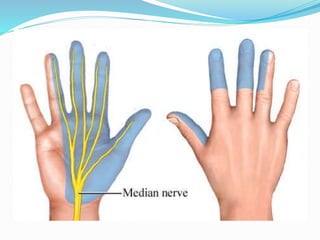
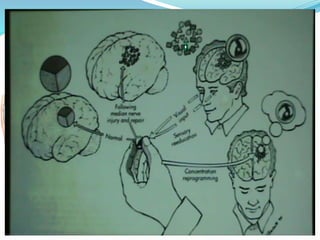
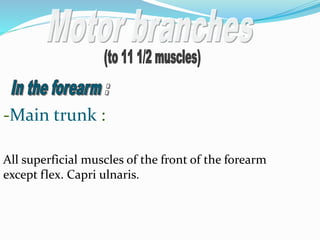
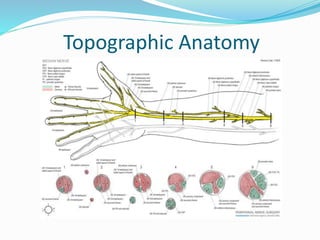












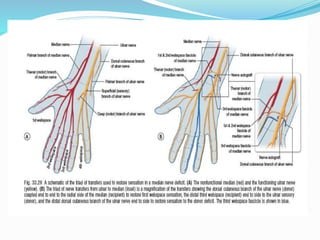



This document provides details on the anatomy, clinical examination, treatment, and tendon transfer procedures for median nerve injuries. It discusses: 1) The anatomy of the median nerve from its origin through the arm, forearm, wrist and hand. 2) Causes of median nerve injuries including trauma, leprosy, and neurological disorders. 3) Clinical signs of median nerve injuries including weakness of thumb opposition and flexion of the wrist. 4) Surgical techniques for median nerve repair and tendon transfers to restore thumb and hand function, including the Royle-Thompson and Burkhalter procedures.
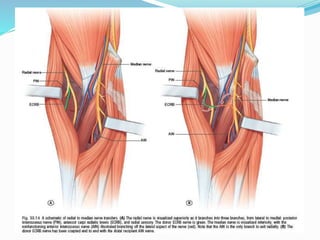
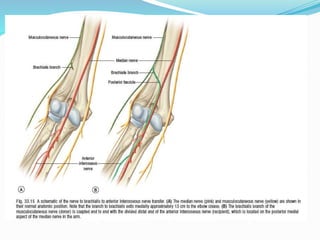
![Peripheral Nerves of Upper Limb [Radial, Median & Ulnar nerve]](https://cdn.slidesharecdn.com/ss_thumbnails/sb-190709091558-thumbnail.jpg?width=640&height=640&fit=bounds)









































































