Downloaded 38 times
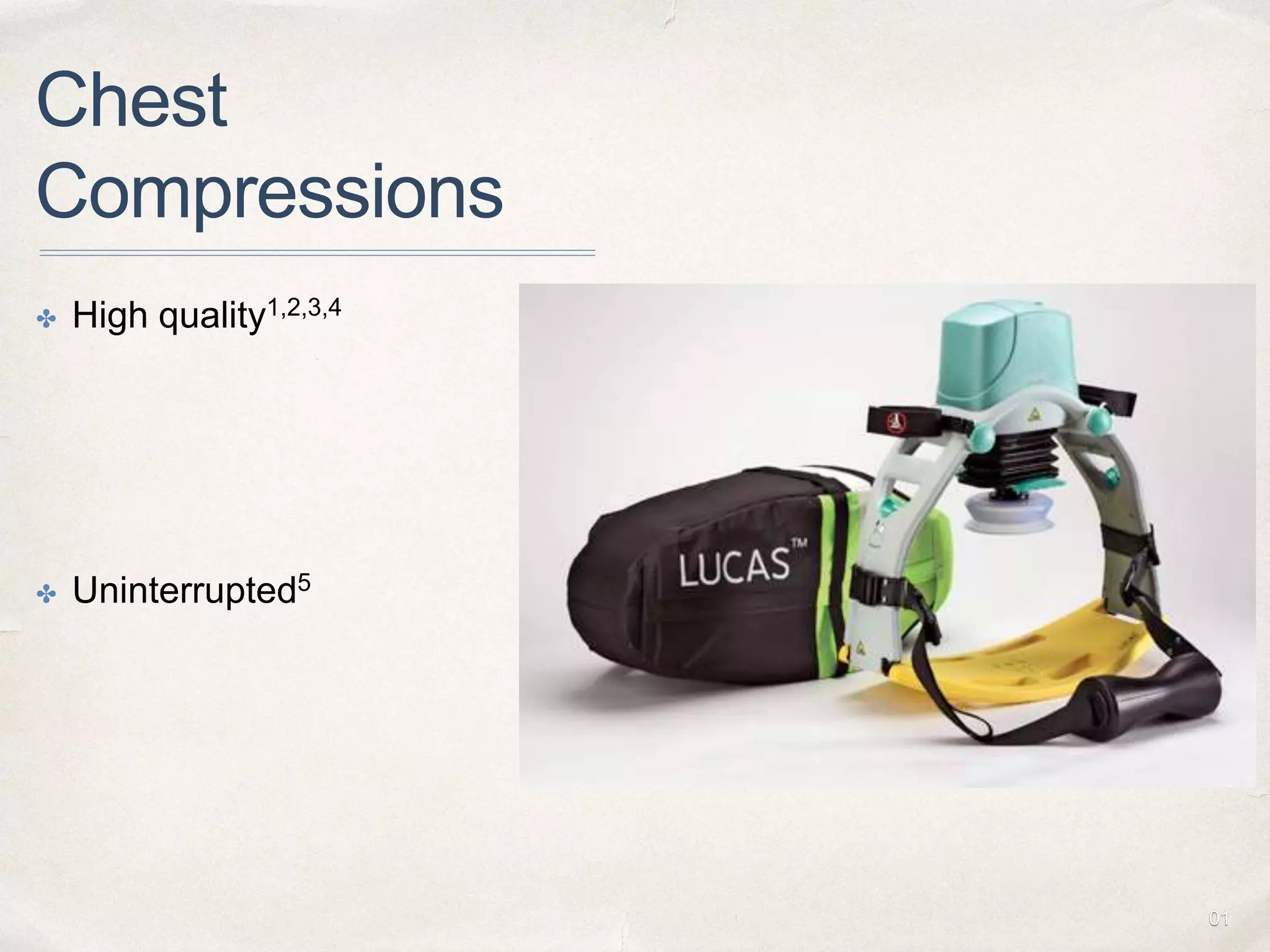
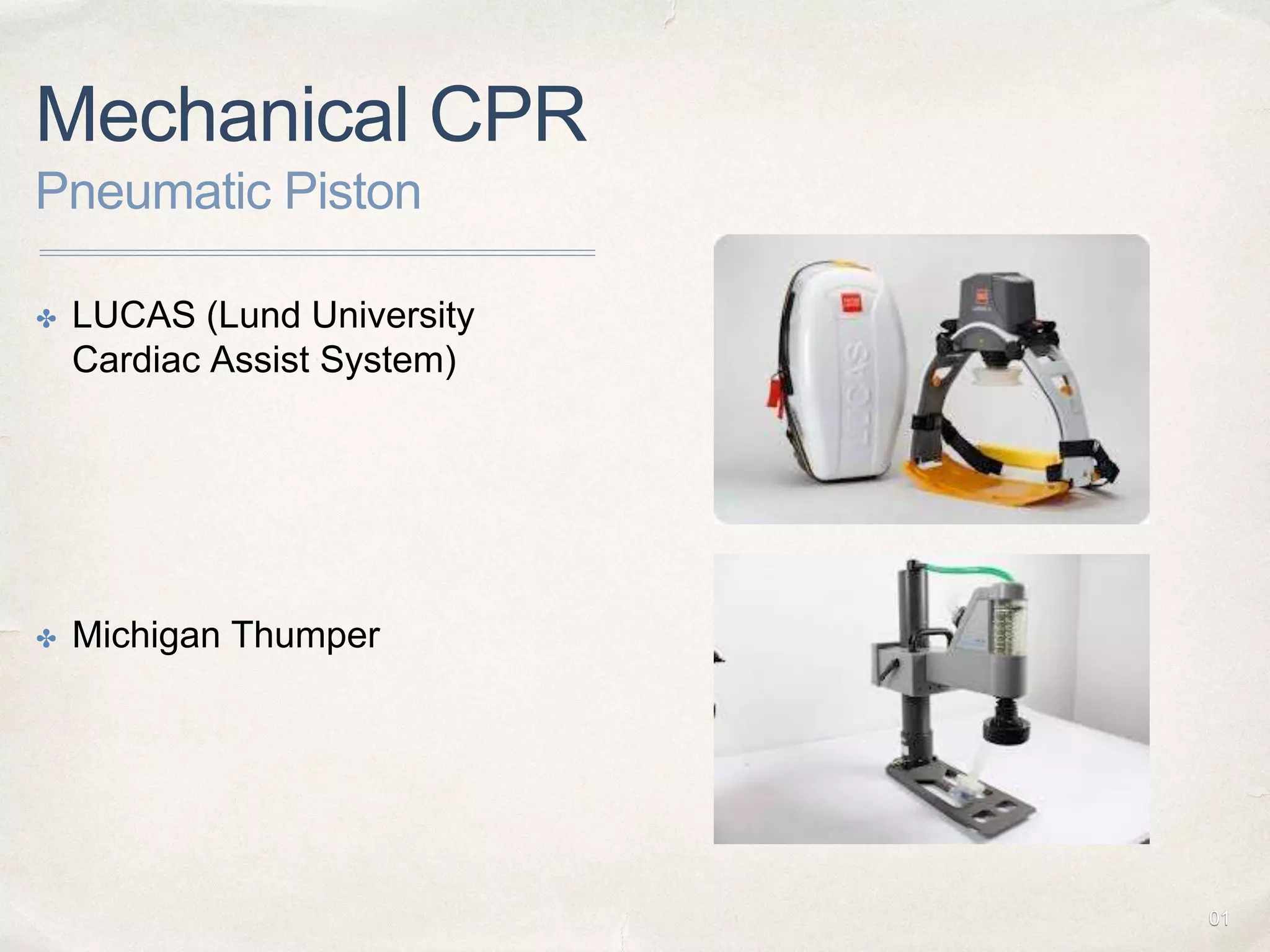
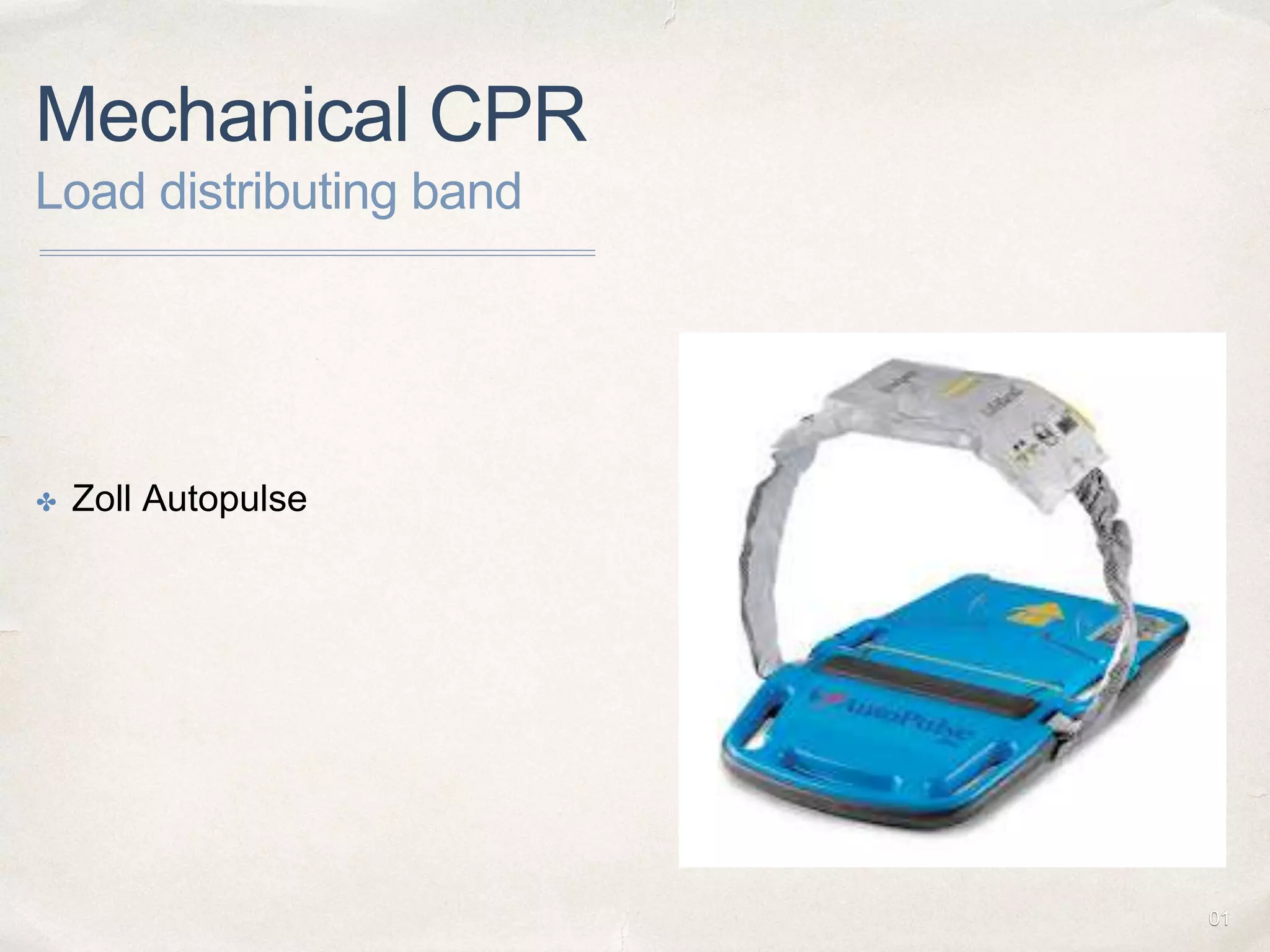
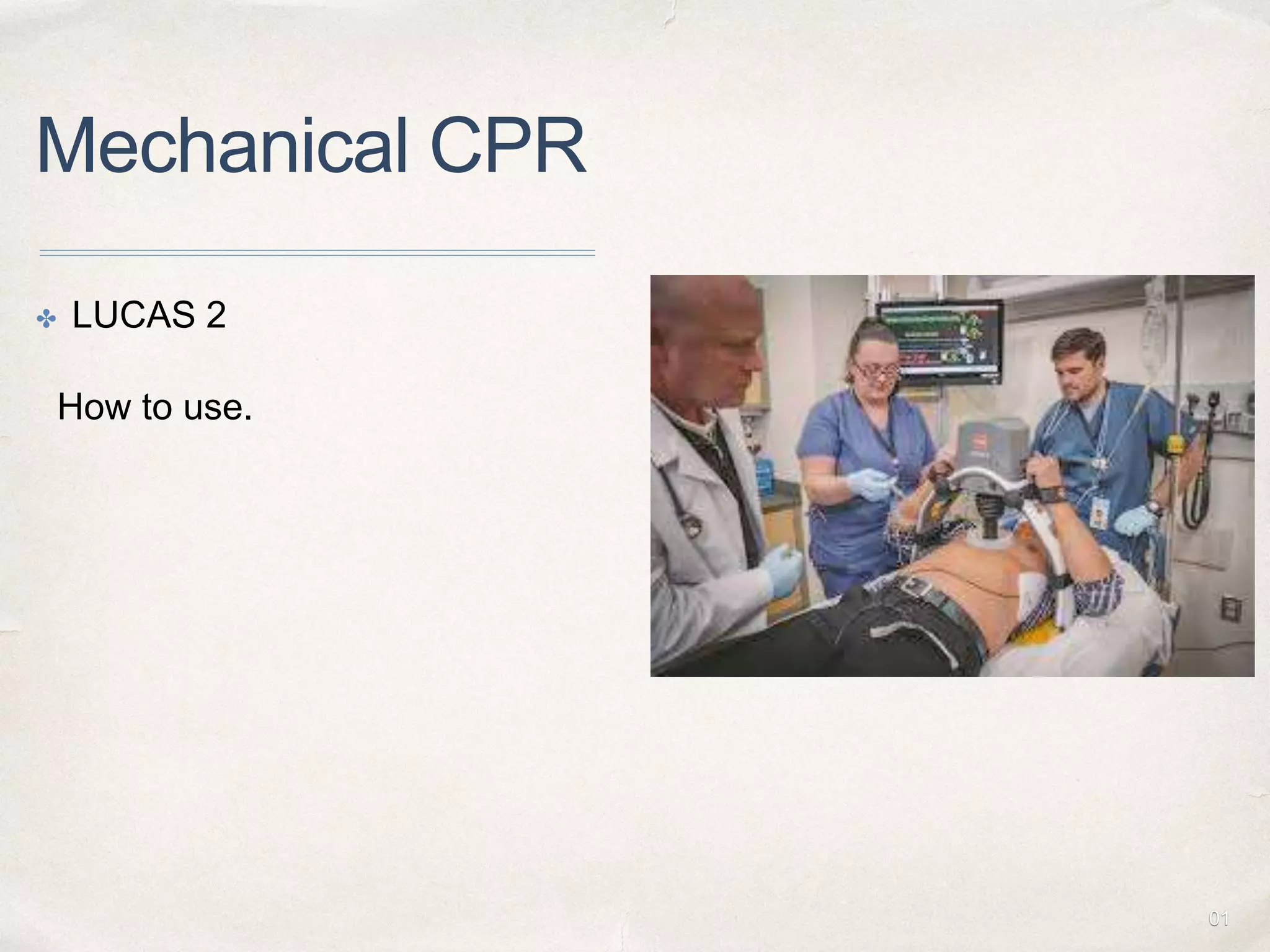

Mechanical CPR devices were developed to address the problems of early fatigue and declining quality of manual chest compressions during prolonged CPR. They work using either a pneumatic piston or load distributing band to provide uninterrupted, consistent chest compressions. Current evidence from meta-analyses shows that mechanical CPR does not provide benefits over manual CPR in terms of ROSC or long-term survival. However, mechanical CPR may be useful in situations where high-quality manual compressions are difficult or when rescuers need to be protected, such as during transfers or prolonged resuscitation efforts. Guidelines do not recommend routine use of mechanical CPR over manual CPR.























































































