Downloaded 13 times

























![CPR Techniques & Devices
(2015 Guidelines)
“The use of mechanical piston devices may be considered
in specific settings where the delivery of high-quality
manual compressions may be challenging or dangerous
for the provider (eg, limited rescuers available, prolonged
CPR, during hypothermic cardiac arrest, in a moving
ambulance, in the angiography suite, during preparation
for extracorporealCPR [ECPR]), provided that rescuers
strictly limit interruptions in CPR during deployment and
removal of the devices.”.](https://image.slidesharecdn.com/2015-cpr-and-ecc-guidelines-update-170531224225/85/CPR-31-320.jpg)
















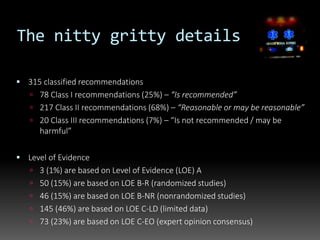
The document summarizes key changes and recommendations from the 2015 American Heart Association (AHA) Resuscitation Guidelines. Some of the major updates include: emphasizing high-quality chest compressions; allowing higher maximum compression rates of 100-120/min; delaying ventilation for initial continuous compressions; and cautioning on prognostication after resuscitation given new therapies. The guidelines are based on an extensive evidence review process involving hundreds of international participants. While manual CPR remains standard, mechanical devices may be considered in specific settings. Areas for further research are identified around physiologic monitoring during CPR and post-resuscitation care.











































































