Downloaded 12 times











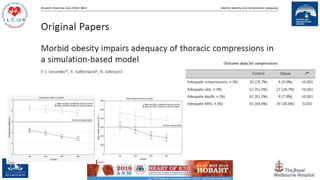
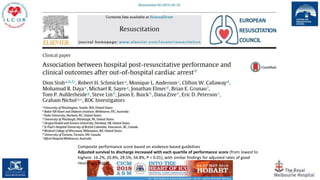
![44
CO-CPR vs. CPR 30:2 (adults)
For bystanders plus dispatcher-instructed CPR, one cohort study[2] of 350,439 mostly adult patients
found that significantly lesspatients receiving CO-CPR experienced favourable neurological outcomes
(RD −0.74, 95% CI: −0.85, −0.63), survived (RD −1.42,95% CI: −1.58, −1.25), and experienced ROSC
(RD −1.62, 95% CI:−1.81, −1.42) compared to CPR 30:2.](https://image.slidesharecdn.com/t19seehtcetw2acduq4r-signature-82eb833951e3665a647e65b0eb18244e85e3976100786ef428e46a6b4c4cc429-poli-180919074733/85/Resuscitation-update-by-Professor-Peter-Morley-44-320.jpg)


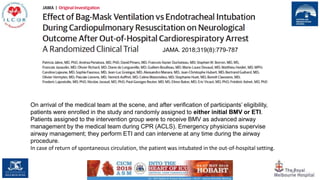
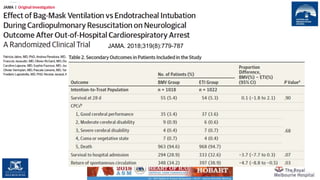
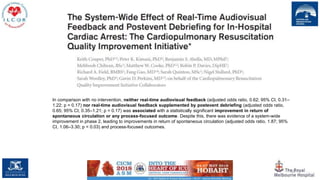
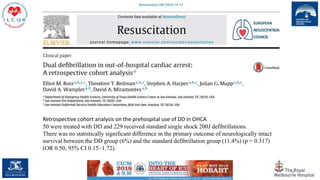
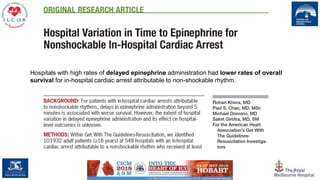
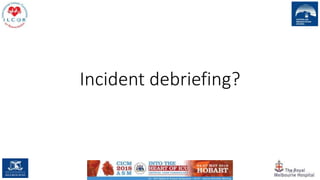
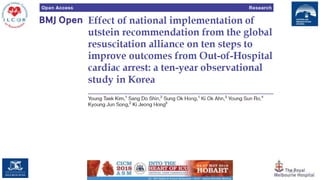
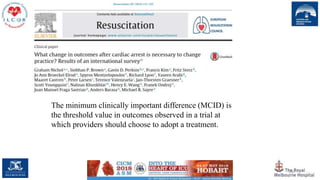
![49
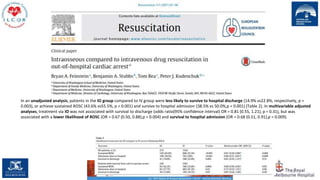
A total of 1129 of 12,613 patients with available data (9.0%) in the intervention group and 1072 of 11,035 with
available data (9.7%) in the control group survived until discharge (difference, −0.7 percentage points; 95%
confidence interval [CI], −1.5 to 0.1; P = 0.07);
7.0% of the patients in the intervention group and 7.7% of those in the control group survived with favorable
neurologic function at discharge (difference, −0.6 percentage points; 95% CI, −1.4 to 0.1, P = 0.09).](https://image.slidesharecdn.com/t19seehtcetw2acduq4r-signature-82eb833951e3665a647e65b0eb18244e85e3976100786ef428e46a6b4c4cc429-poli-180919074733/85/Resuscitation-update-by-Professor-Peter-Morley-49-320.jpg)




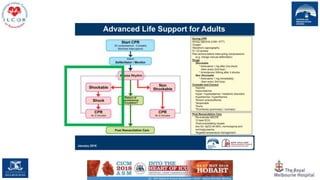

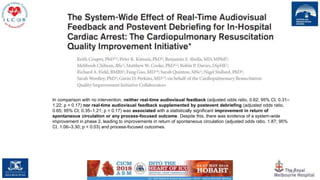
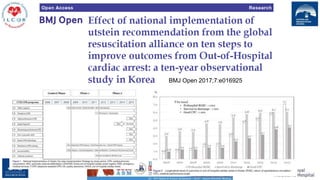
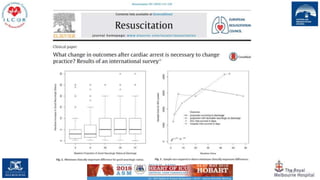
![64
Meta-analysis of 6 observational studies without critical risk of bias showed that bystander AED use was
associated with survival to hospital discharge (all rhythms OR: 1.73 [95%CI: 1.36, 2.18], shockable
rhythms OR: 1.66 [95%CI: 1.54, 1.79]) and favorable neurological outcome (all rhythms OR: 2.12
[95%CI: 1.36, 3.29], shockable rhythms OR: 2.37 [95%CI: 1.58, 3.57]).
However, the overall quality of evidence was low to very low.](https://image.slidesharecdn.com/t19seehtcetw2acduq4r-signature-82eb833951e3665a647e65b0eb18244e85e3976100786ef428e46a6b4c4cc429-poli-180919074733/85/Resuscitation-update-by-Professor-Peter-Morley-64-320.jpg)







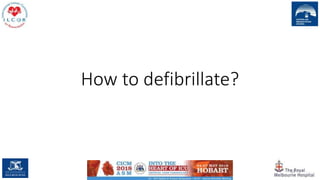
![100
Twenty-three patients were enrolled in our study. The mean duration of pulse checks with Point-Of-Care
Ultra-Sound (POCUS) was 21.0 s (95% CI, 18–24) compared with 13.0 s (95% CI, 12–15) for those without
POCUS.
POCUS increased the duration of pulse checks and CPR interruption by 8.4 s (95% CI, 6.7–10.0 [p <
0.0001]).](https://image.slidesharecdn.com/t19seehtcetw2acduq4r-signature-82eb833951e3665a647e65b0eb18244e85e3976100786ef428e46a6b4c4cc429-poli-180919074733/85/Resuscitation-update-by-Professor-Peter-Morley-100-320.jpg)


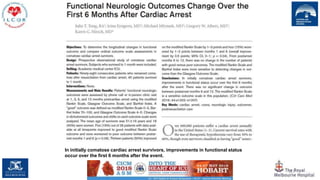
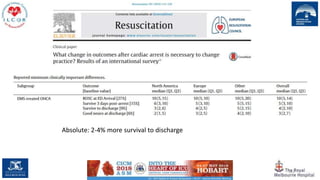
![We have learnt not to stop too soon
109
Compared with patients at hospitals in the quartile with
the shortest median resuscitation attempts in non-survivors
(16 min [IQR 15–17]), those at hospitals in the quartile
with the longest attempts (25 min [25–28]) had a higher
likelihood of return of spontaneous circulation (adjusted
risk ratio 1.12, 95% CI 1.06–1.18; p<0.0001) and survival to
discharge (1.12, 1.02–1.23; 0.021).](https://image.slidesharecdn.com/t19seehtcetw2acduq4r-signature-82eb833951e3665a647e65b0eb18244e85e3976100786ef428e46a6b4c4cc429-poli-180919074733/85/Resuscitation-update-by-Professor-Peter-Morley-109-320.jpg)







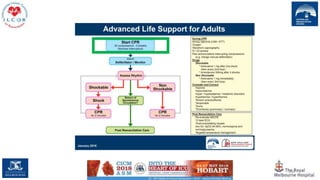
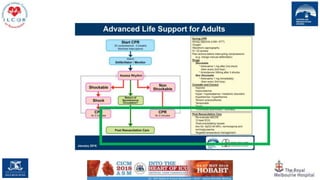




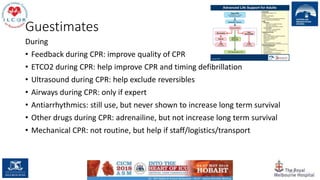
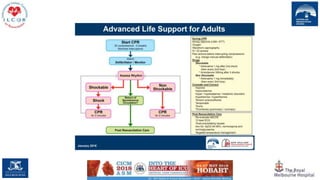




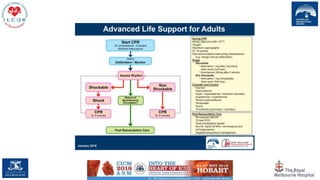
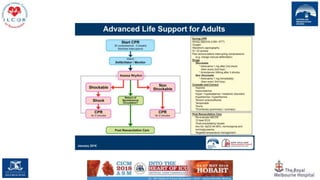
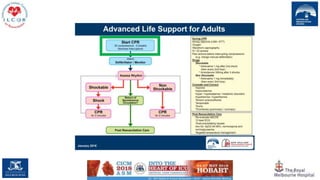
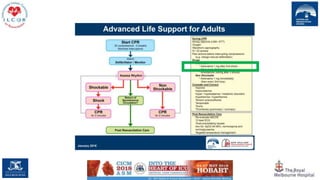
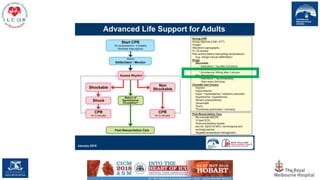
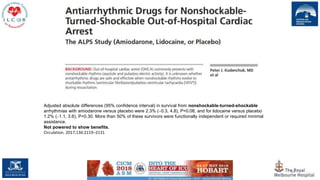
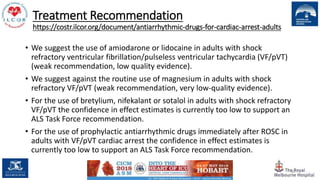
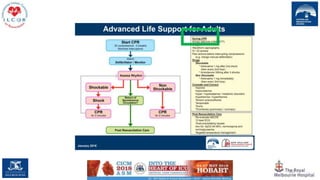
This document provides updates on resuscitation guidelines based on ongoing evaluations of new evidence and treatment recommendations. It discusses the roles of various techniques and interventions during cardiac arrest, emphasizing the significance of continuous chest compressions and the implications of different medications and devices used. Furthermore, it highlights the current concerns and insights into clinical practices in resuscitation and the necessity for ongoing research in this field.













































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)









