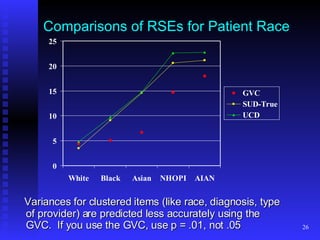
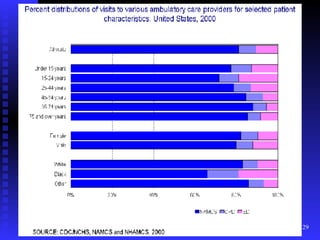
This document provides an overview of a hands-on workshop for understanding and using data from the National Ambulatory Medical Care Survey (NAMCS) and the National Hospital Ambulatory Medical Care Survey (NHAMCS). The workshop covers survey background and data uses, technical considerations, accessing the data online, using raw data files, and advanced topics. NAMCS and NHAMCS collect data on visits to office-based physicians and hospital outpatient/emergency departments, including patient characteristics, visit details, provider information, and mentions of up to six medications per visit.