Downloaded 53 times
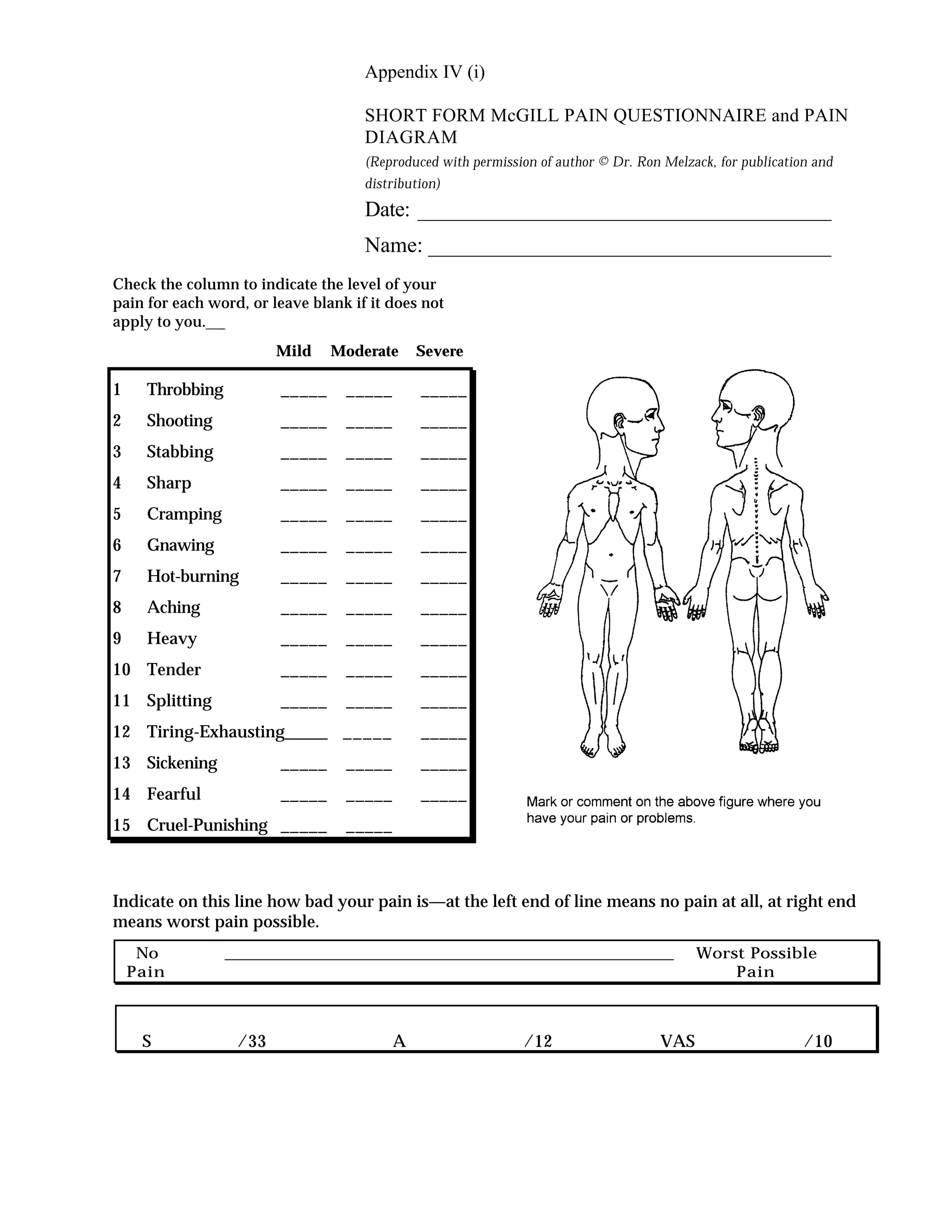

The document is a short form McGill Pain Questionnaire used to assess a patient's level of pain. It contains 15 words to describe types of pain that the patient rates on a scale of mild, moderate, or severe. It also includes a visual analog scale to rate the overall intensity of their pain from no pain to worst possible pain.










































































![Exame neuro infantil[1].2](https://cdn.slidesharecdn.com/ss_thumbnails/exameneuroinfantil1-2-120322123912-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)

























![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)
