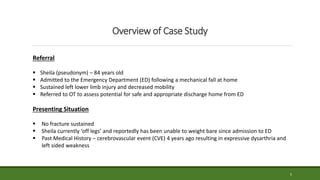
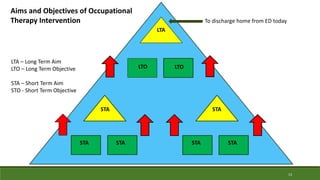
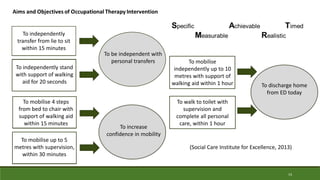
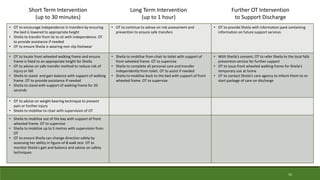
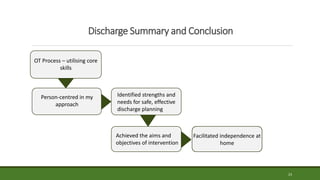
This document provides a case study of an occupational therapy assessment and intervention for an 84-year-old woman admitted to the emergency department following a fall at home. The occupational therapist assessed the woman's mobility, transfers, and ability to complete activities of daily living to determine if she could be safely discharged home. Short term goals were set for the woman to increase her mobility and confidence, which were achieved within 30-60 minutes. Referral to falls prevention services was also made. The assessment and intervention demonstrated the role of occupational therapy in facilitating safe, independent discharge from the emergency department.

![References
Bissett, M., Cusick, A. and Lannin, N.A. (2013) ‘Functional assessments utilised in emergency
departments: a systematic review’, Age and Ageing, 42(2), pp.163-172.
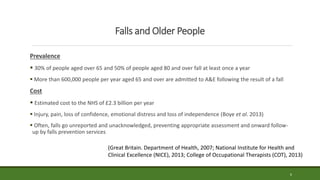
Boye, N., Van Lieshout, E., Van Beeck, E., Hartholt, K., Van der Cammen, T. and Patka, P. (2013)
‘The impact of falls in the elderly’, Trauma, 15(1), pp.29-35.
Campbell, A.J. and Robertson, M.C. (2013) ‘Fall prevention: single or multiple interventions?
Single interventions for fall prevention’, Journal of the American Geriatrics Society, 61(2), pp.281-
287.
College of Occupational Therapists (2010) Code of ethics and professional conduct [Online].
Available at: http://www.cot.co.uk/sites/default/files/publications/public/Code-of-
Ethics2010.pdf. (Accessed: 15 June 2014).
College of Occupational Therapists (2013) Falls management. London: COT.
26](https://image.slidesharecdn.com/40bb1c33-ba81-4b25-af10-ad5905cc66c5-160206123532/85/OCT305-Case-Study-Presentation-10230458-26-320.jpg)
![27
Cusick, A., Johnson, L. and Bissett, M. (2009) ‘Occupational therapy in emergency departments:
Australian practice’, Journal of Evaluation in Clinical Practice, 15(2), pp.257-265.
Great Britain. Department of Health (2001) National Service Framework for older people
[Online]. Available at: http://www.apllg.eu/resources/NSF+for+Older+People.pdf. (Accessed:
12 June 2014).
Great Britain. Department of Health (2007) Urgent care pathways for older people with complex
needs: best practice guidance [Online]. Available at: http://www.em-
online.com/download/medical_article/36261_Older%20People%20Complex%20Needs.pdf.
(Accessed: 12 June 2014).
Health and Care Professions Council (2012) Standards of conduct, performance and ethics
[Online]. Available at: http://www.hpc-
uk.org/assets/documents/10003B6EStandardsofconduct,performanceandethics.pdf.
(Accessed: 15 June 2014).
Jones, D. and Whitaker, T. (2011) ‘Preventing falls in older people: assessment and
interventions’, Nursing Standard, 25(52), pp.50-55.](https://image.slidesharecdn.com/40bb1c33-ba81-4b25-af10-ad5905cc66c5-160206123532/85/OCT305-Case-Study-Presentation-10230458-27-320.jpg)
![28
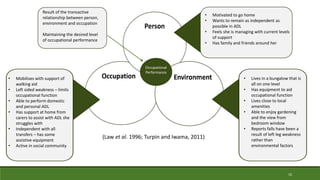
Law, M., Cooper, B,. Strong, S., Stewart, D., Rigby, P. and Letts, L. (1996) ‘The Person-
Environment-Occupation Model: a transactive approach to occupational performance’,
Canadian Journal of Occupational Therapy, 63(1), pp.9-23.
Lee, D., McDermott, F., Hoffman, T. and Haines, T. (2013) ‘They will tell me if there is a problem’:
limited discussion between health professionals, older adults and their caregivers on falls
prevention during and after hospitalization’, Health Education Research, 28(6), pp.1051-1066.
Logan, P., Coupland, C., Gladman, J., Sahoto, O., Stoner-Hobbs, V., Robertson, K., Tomlinson, V.,
Ward, M., Sach, T. and Avery, A. (2010) ‘Community falls prevention for people who call an
emergency ambulance after a fall: randomised controlled trial’, British Medical Journal, 340.
[Online] DOI: http://dx.doi.org/10.1136/bmj.c2102. (Accessed: 13 June 2014).
Maclean, F., Carin-Levy, G., Hunter, H., Malcolmson, L. and Locke, E. (2012) ‘The usefulness of
the Person-Environment-Occupation Model in an acute physical health care setting’, British
Journal of Occupational Therapy, 75(12), pp.555-562.
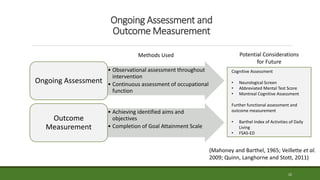
Mahoney, F.I. and Barthel, D.W. (1965) ‘Functional evaluation: the Barthel Index’, Maryland State
Medical Journal, 14, pp.61-65.](https://image.slidesharecdn.com/40bb1c33-ba81-4b25-af10-ad5905cc66c5-160206123532/85/OCT305-Case-Study-Presentation-10230458-28-320.jpg)