
Downloaded 117 times


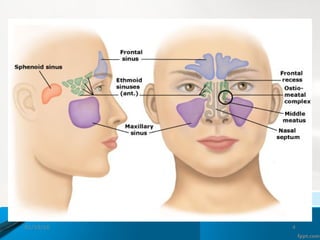







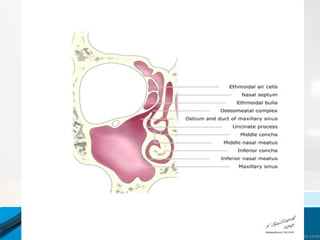


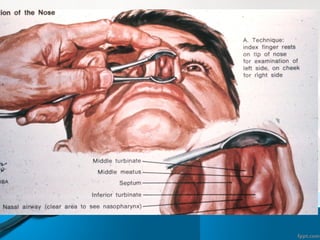
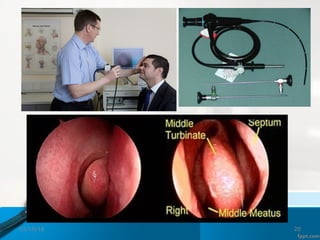

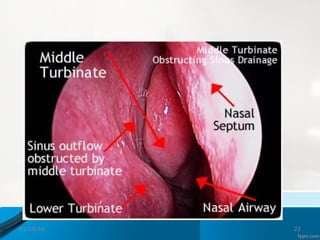
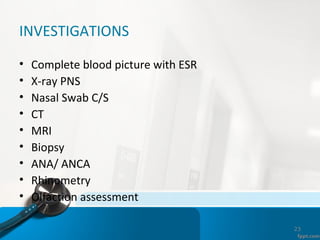






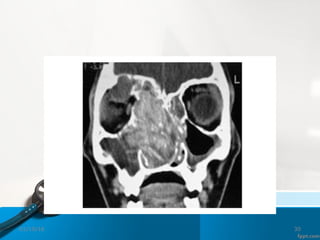












This document provides an overview of rhinosinusitis, including its classification, epidemiology, pathogenesis, signs and symptoms, investigations, complications, and management. It discusses the four paranasal sinuses and defines acute, recurrent acute, and chronic rhinosinusitis. Common predisposing factors and pathogens are outlined. Examination techniques like anterior rhinoscopy and nasoendoscopy are described. Investigations may include blood tests, sinus x-rays, CT scans, and biopsies. Management involves initial conservative treatments like antibiotics, steroids, and sinus irrigation, with surgical options like FESS for refractory cases.






































































![Introduction to hearing implairment & cochlear implantation]](https://cdn.slidesharecdn.com/ss_thumbnails/introductiontohearingimplairmentcochlearimplantation-161111054000-thumbnail.jpg?width=640&height=640&fit=bounds)




































