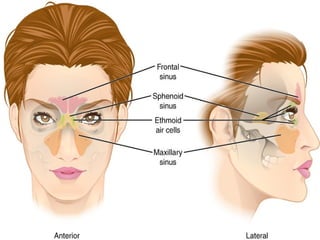
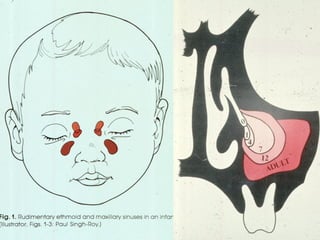
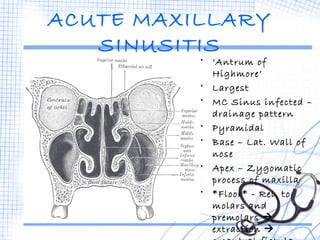
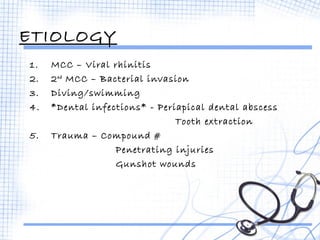
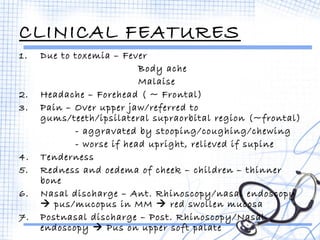
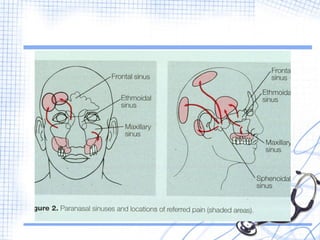
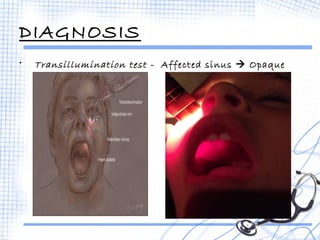
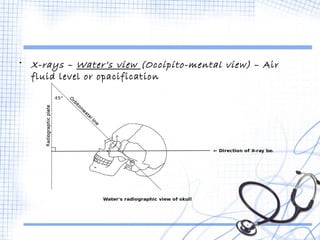
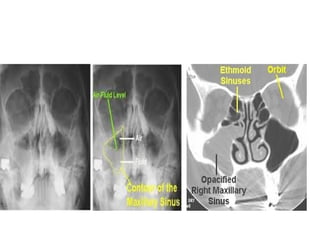
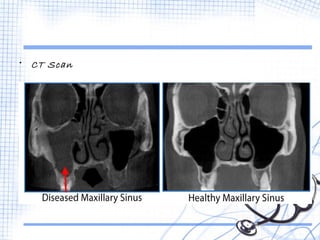
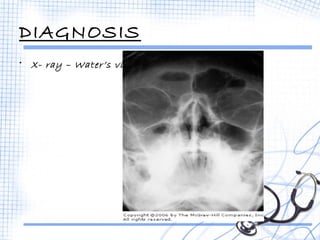
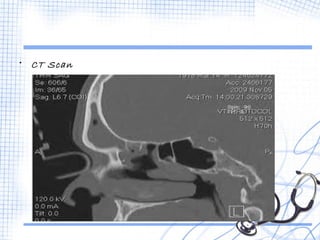
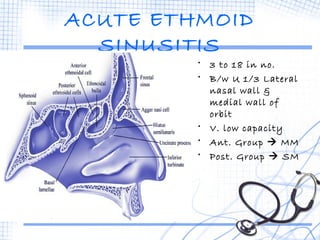
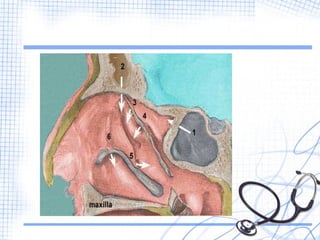
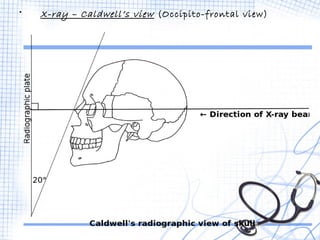
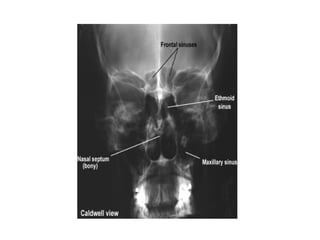
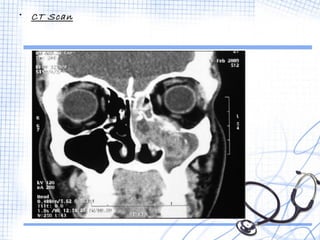
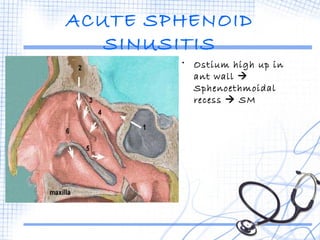
This document discusses the embryology, anatomy, and clinical presentation of acute sinusitis. It begins by describing the development of the paranasal sinuses from pouches in the nasal cavity between 3-5 months of gestation. It then covers the specific anatomy and development of the maxillary, frontal, ethmoid, and sphenoid sinuses. The document discusses the causes, symptoms, diagnoses, and potential complications of acute sinusitis involving each sinus. Common symptoms include headache, facial pain, and nasal discharge. Diagnosis involves transillumination, x-rays such as Waters' view, and CT scans. Complications can include orbital or brain infections if the condition worsens or goes untreated.