Downloaded 36 times


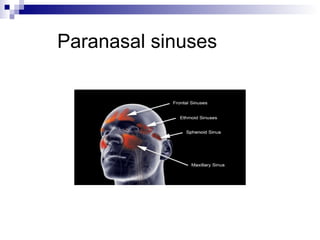
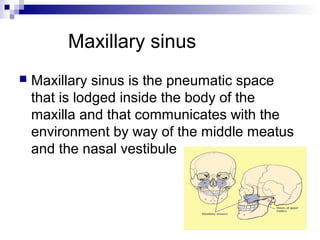

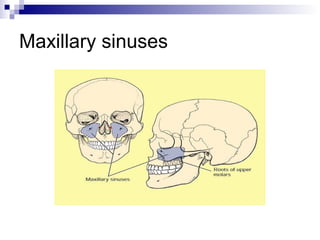
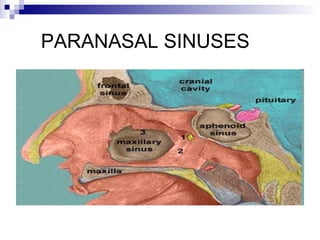

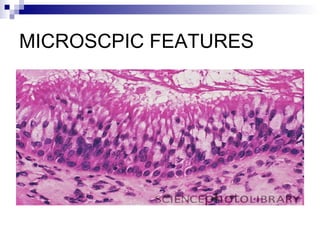
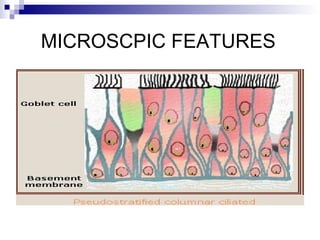
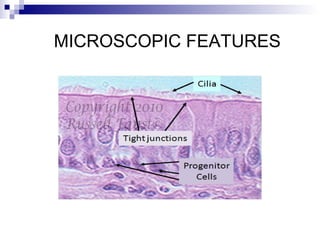
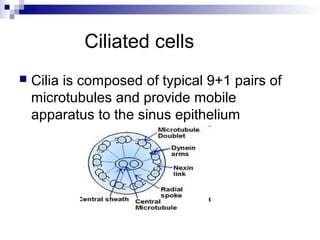

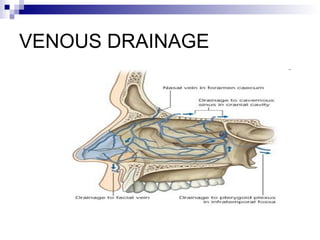
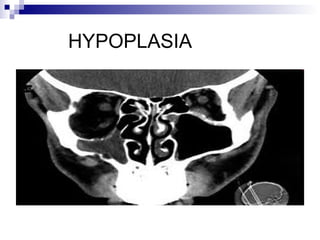
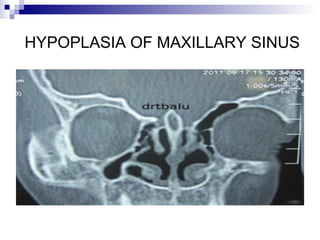
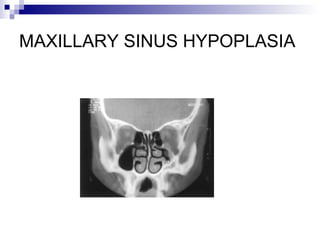
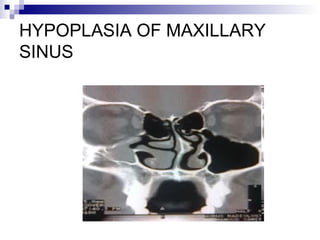

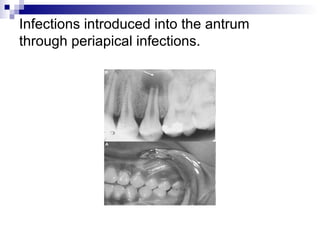
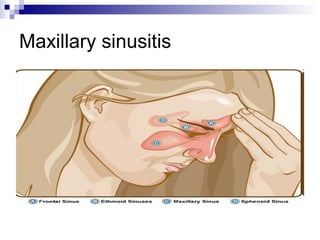

The document provides an extensive overview of the paranasal sinuses, specifically detailing the maxillary sinuses, their anatomy, structure, and functions. It discusses the processes of pneumatization, microscopic features, and the sinus's clinical significance, including common conditions such as maxillary sinusitis, its causes, and complications related to dental procedures. Additionally, it highlights the anatomical relationships and implications of infections, emphasizing the importance of understanding sinus anatomy in dentistry and maxillofacial surgery.































































































