This document provides information about the maxillary sinus, including its definition, development, structure, blood and nerve supply, microscopic features, functions, and clinical importance. Some key points:
- The maxillary sinus is the largest paired sinus, located within the body of the maxilla.
- It begins developing at 12 weeks of fetal life and increases in size after birth. Abnormalities can cause developmental issues.
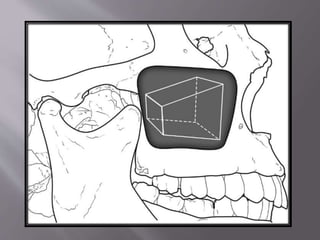
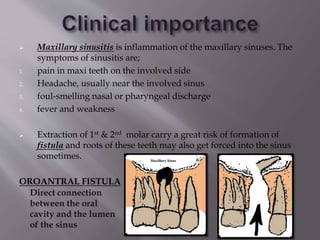
- It has a four-sided pyramid shape and borders the maxilla, orbit, and alveolar process. Thin bone often separates it from upper molars/premolars.
- Symptoms of maxillary sinusitis include pain, headache, nasal discharge, and fever.