





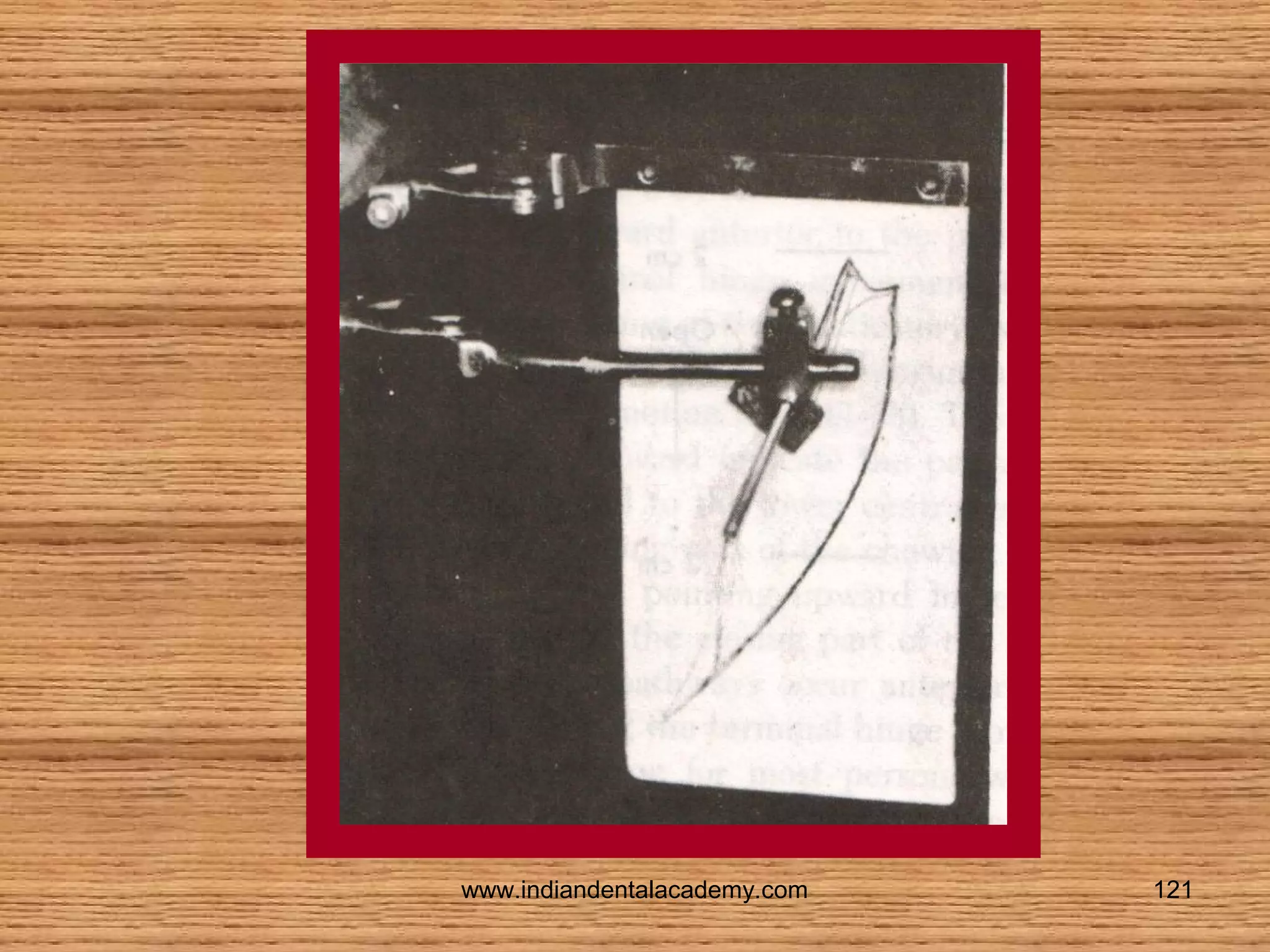
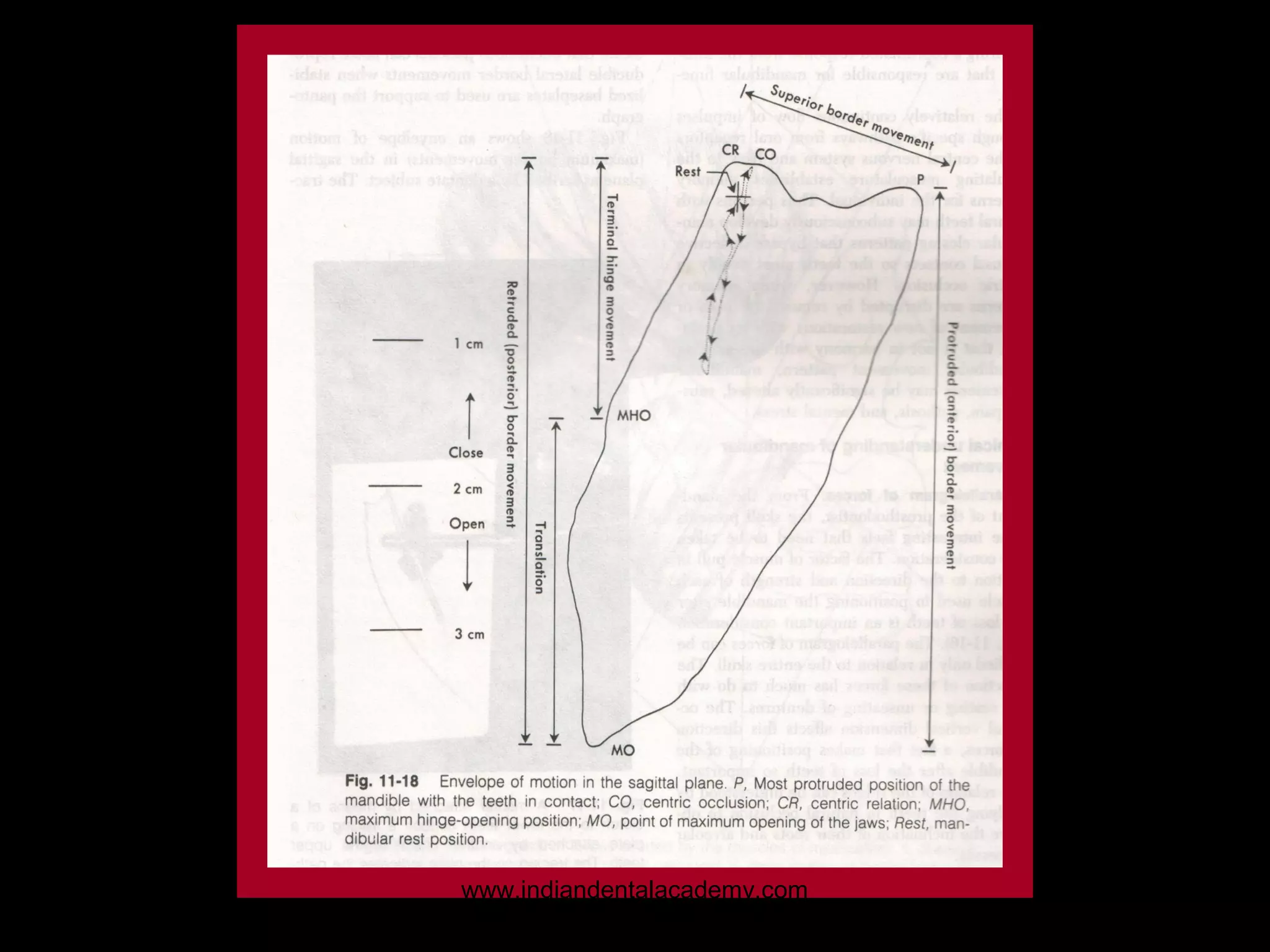
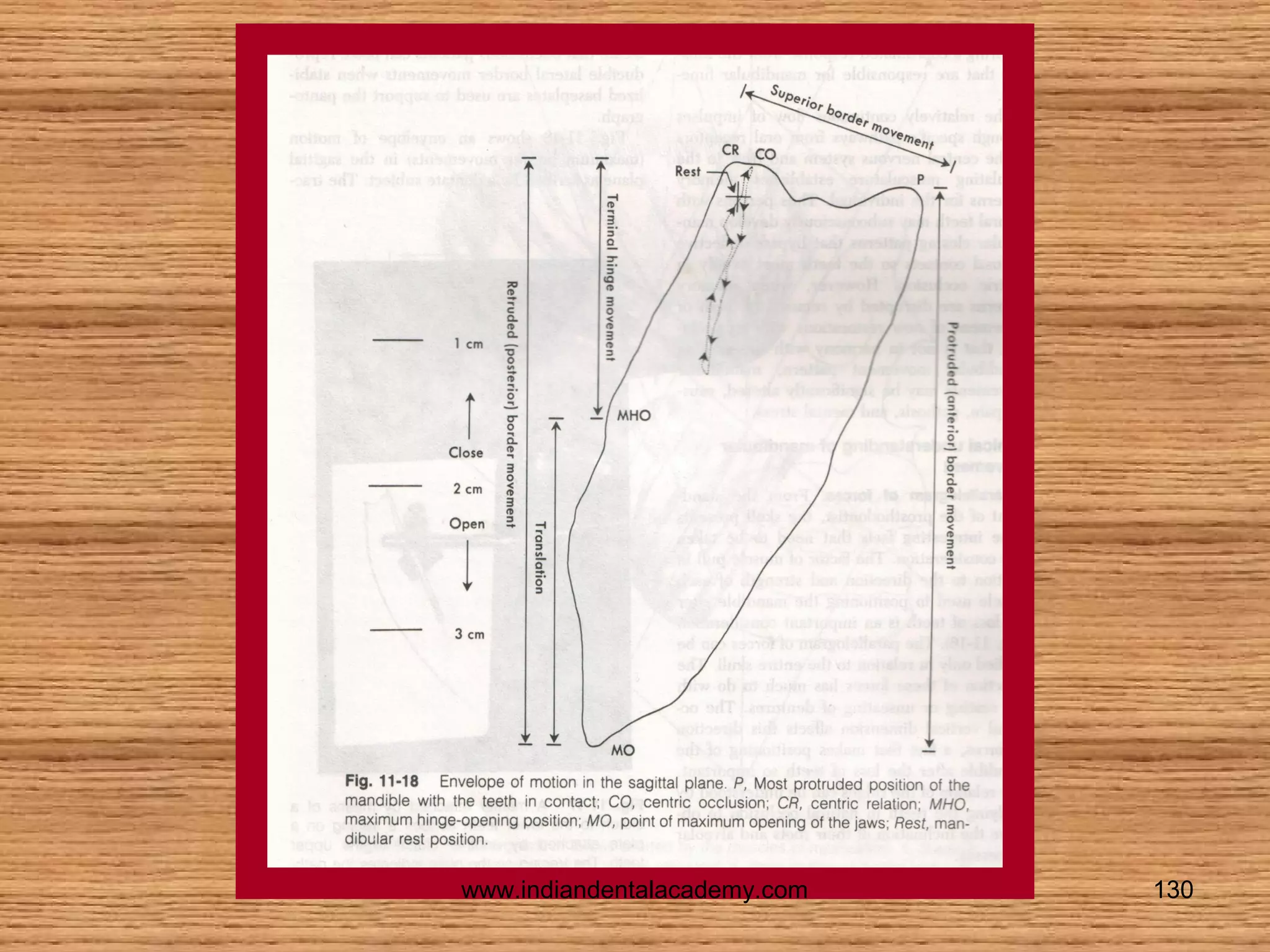
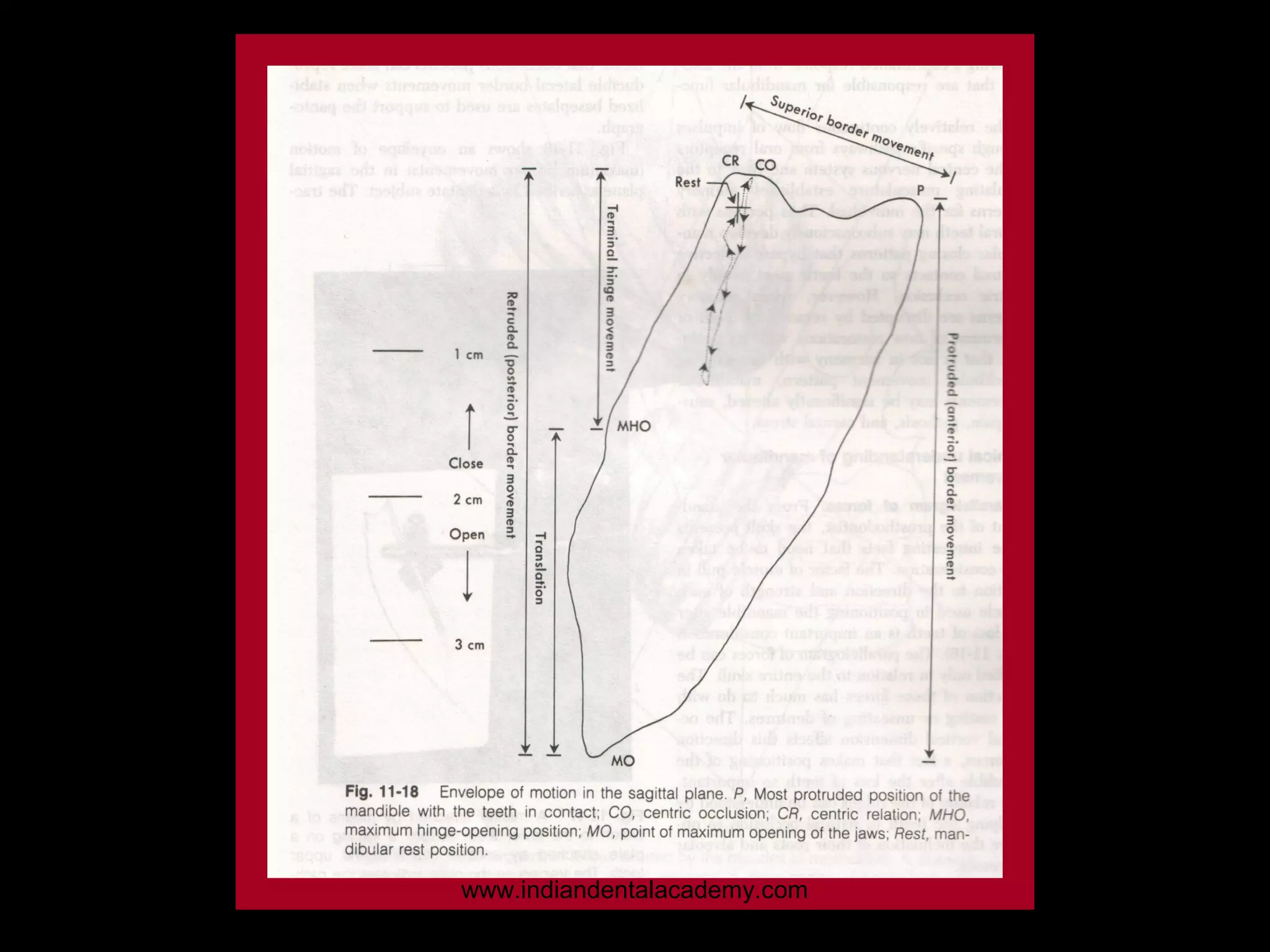
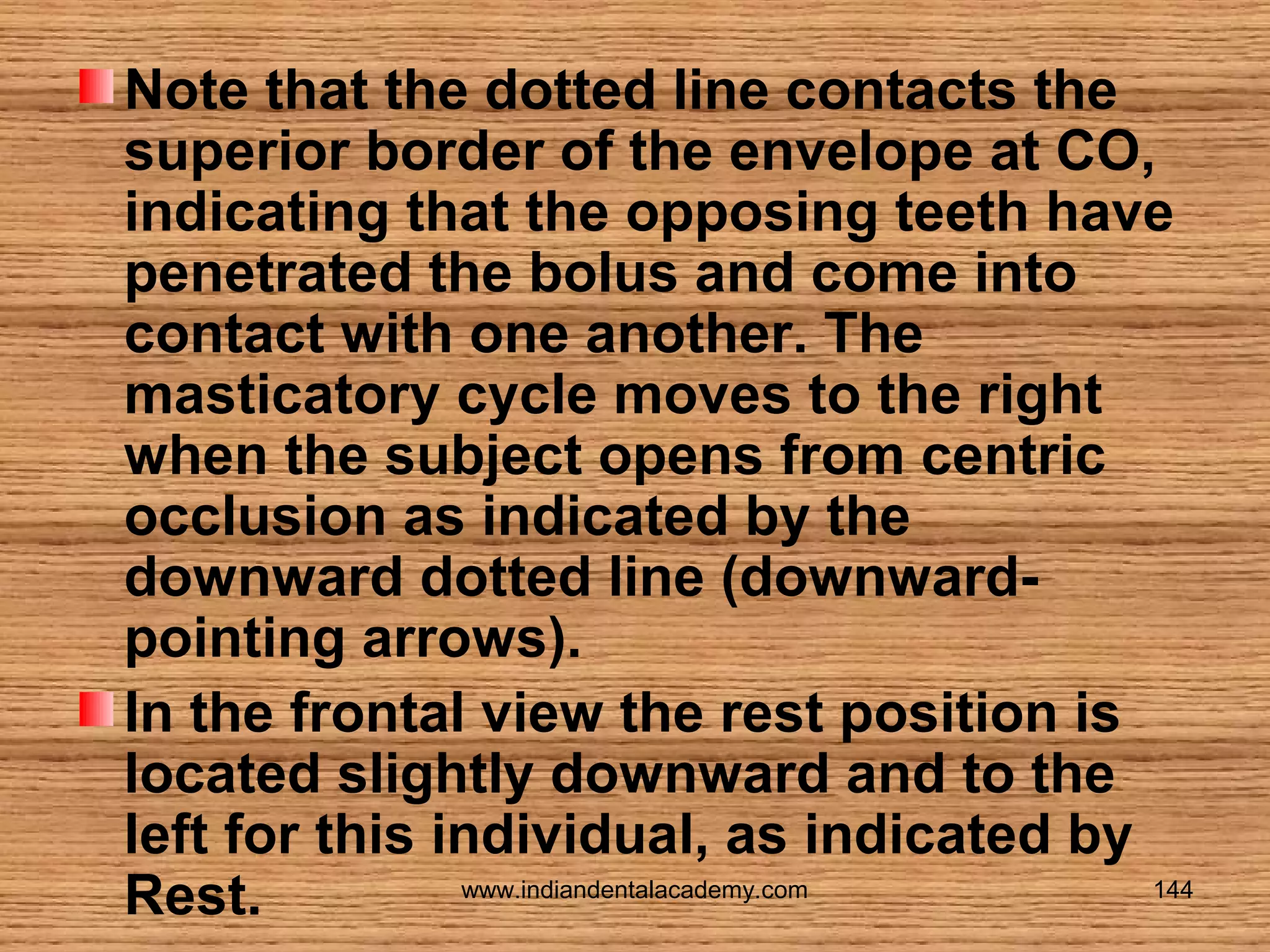
![Fig shows an envelope of motion (maximum border
movements) in the sagittal plane as described by a
www.indiandentalacademy.com
122
dentate subject.]](https://image.slidesharecdn.com/mandibularmovements-140125020437-phpapp01/75/Mandibular-movements-fixed-orthodontic-courses-122-2048.jpg)

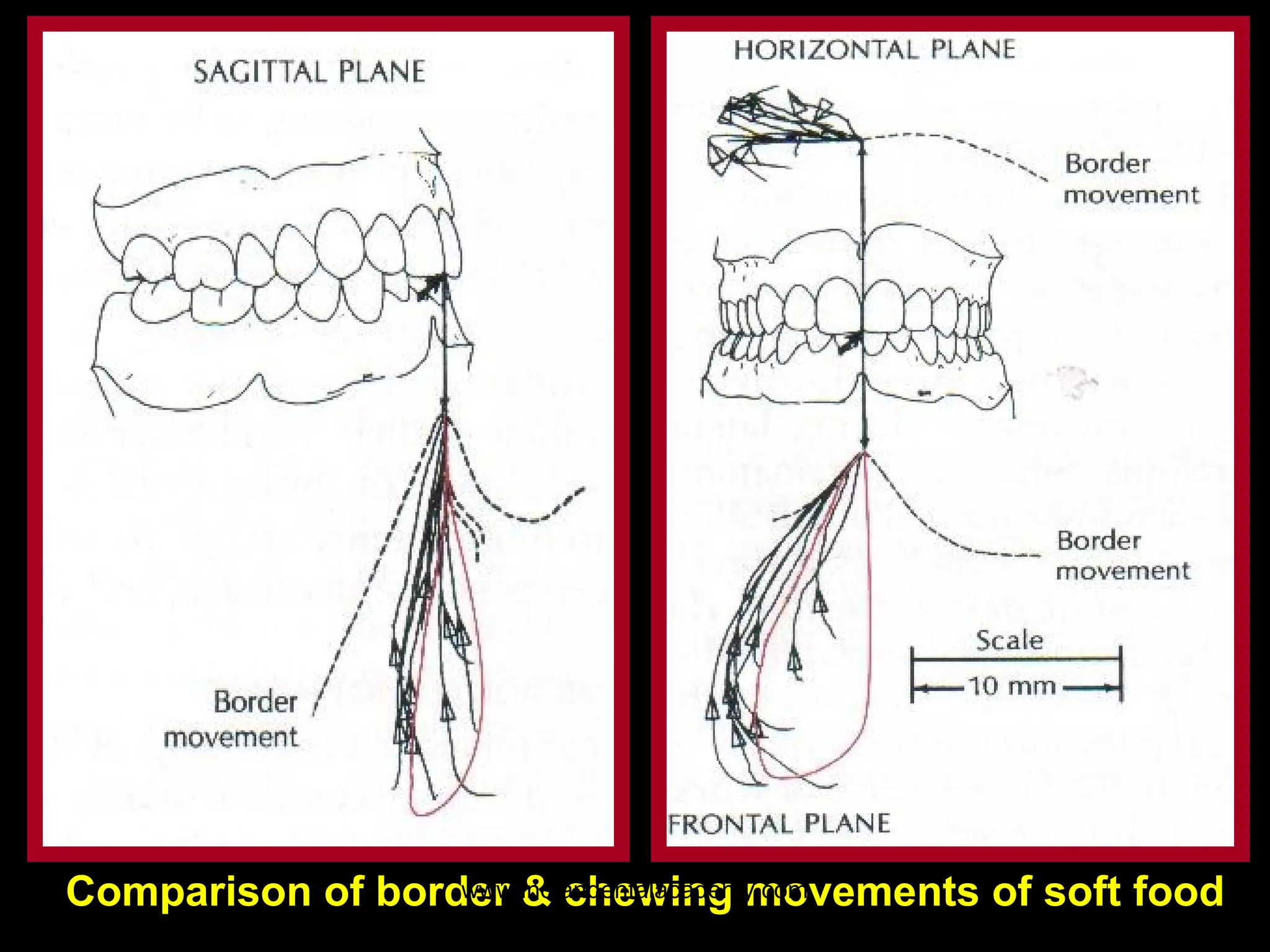
The document provides an extensive overview of mandibular movements, detailing the complex and variable motions of the jaw necessary for functions like speech and mastication. It describes various types of movements such as habitual, border, protrusive, and lateral movements, while also discussing the anatomy of the mandible and its interactions with temporomandibular joints and associated muscles. Important concepts like Bennett movement and mandibular translation are also explored in relation to the mechanics and physiology of jaw movements.











































































































