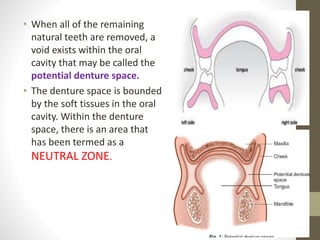
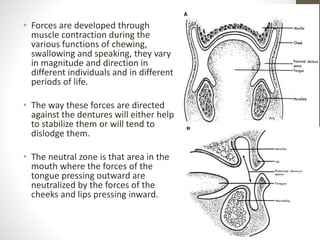
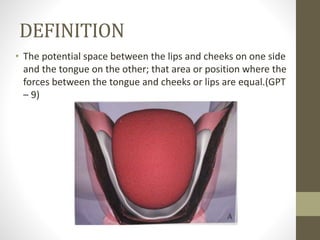
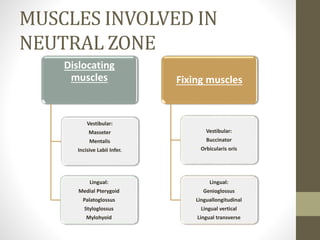
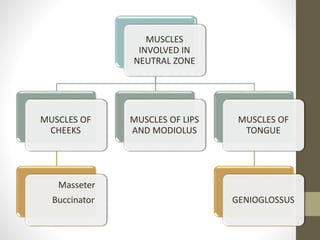
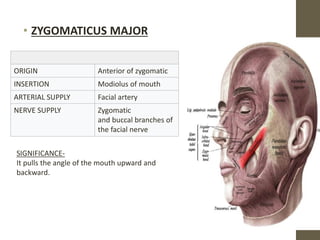
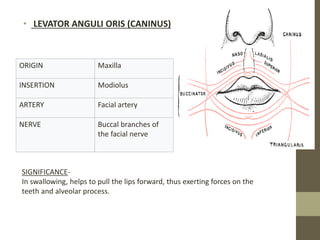
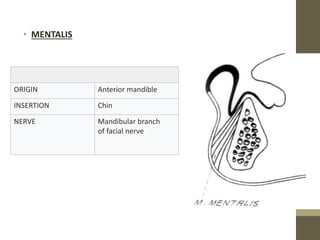
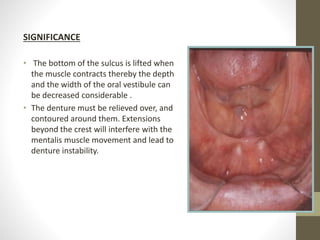
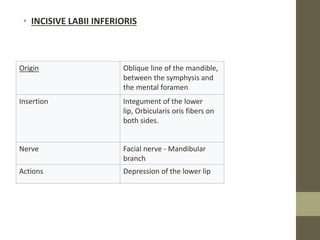
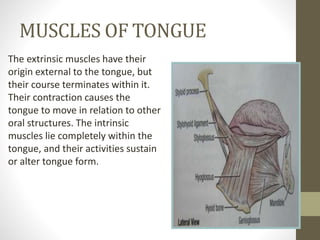
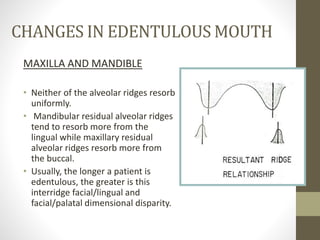
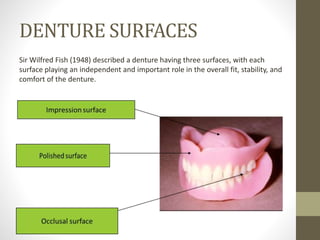
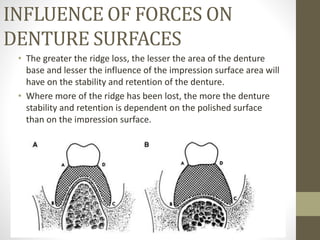
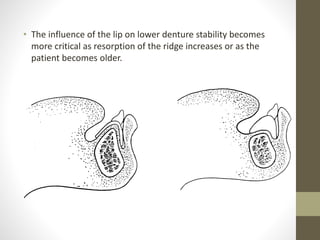
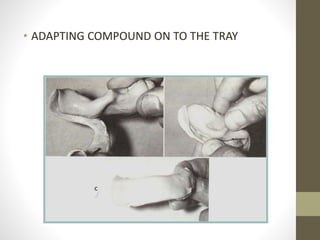
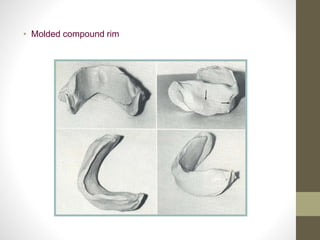
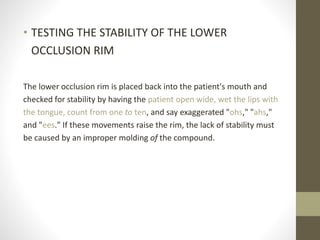
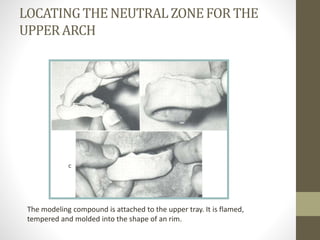
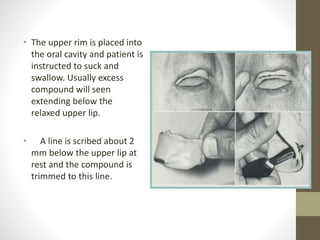
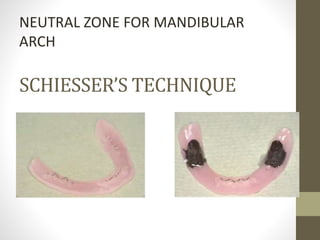
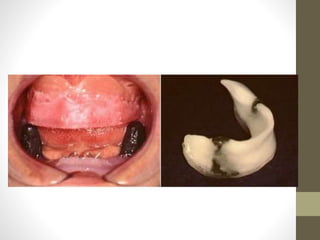
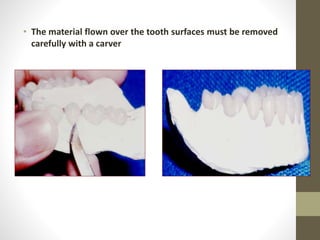
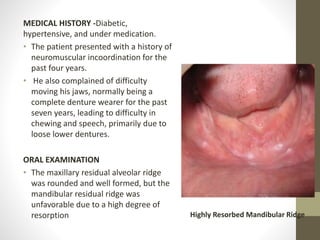
This document discusses the neutral zone in complete dentures. It defines the neutral zone as the area in the mouth where forces from the tongue pressing outward are balanced by forces from the cheeks and lips pressing inward. It describes the muscles involved and how their forces influence tooth position and denture stability. It also discusses how the edentulous mouth changes over time, increasing the importance of properly recording the neutral zone for complete denture fabrication.








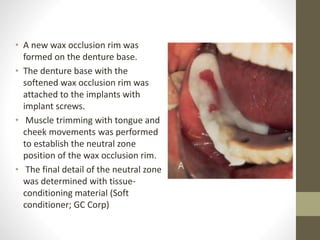































![Stability in Complete Denture [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/stabilityincompletedentureautosaved-260115125839-4ff5a430-thumbnail.jpg?width=640&height=640&fit=bounds)


















































