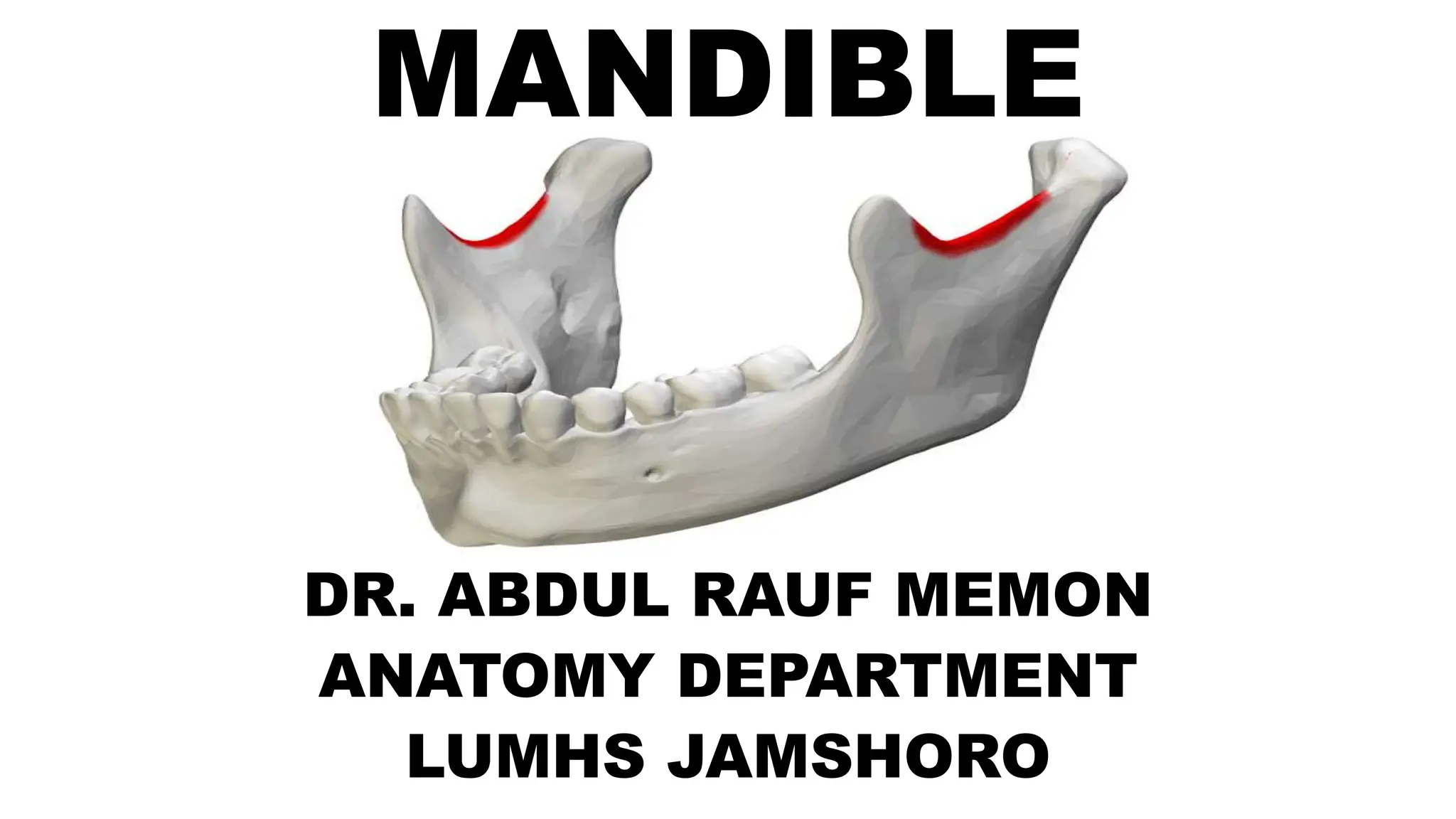
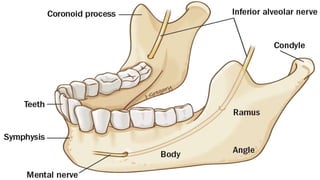
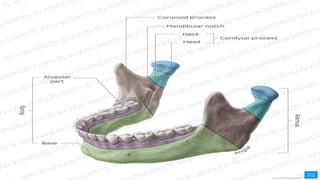
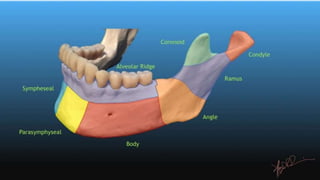
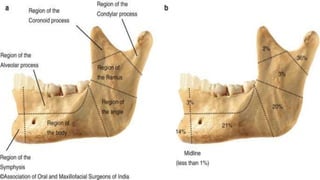
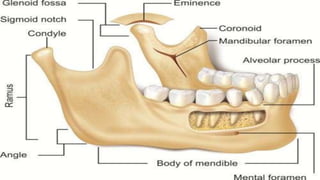
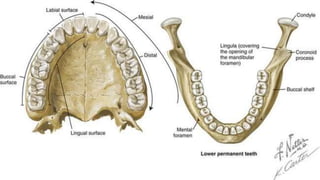
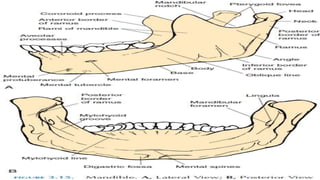
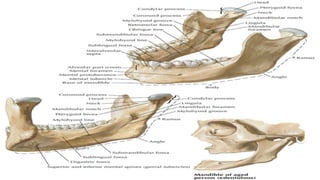
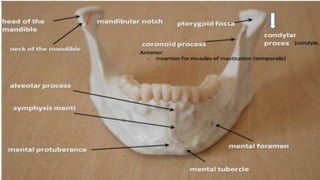
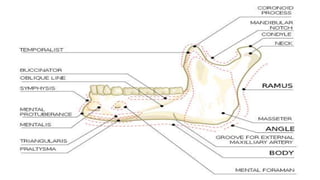
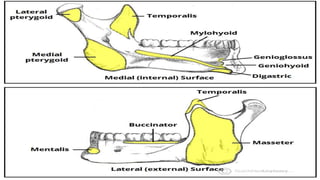
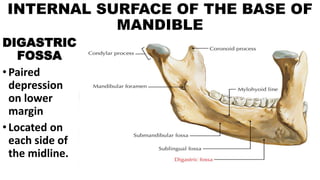
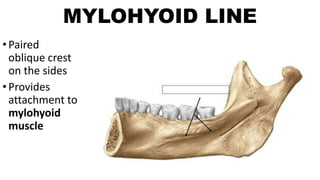
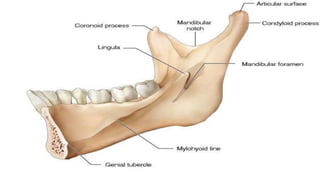
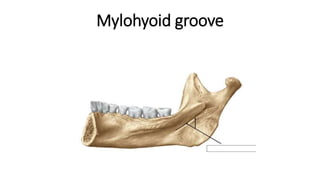
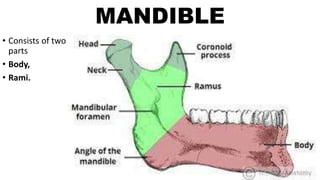
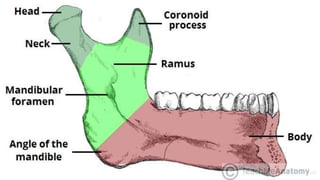
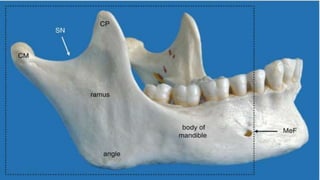
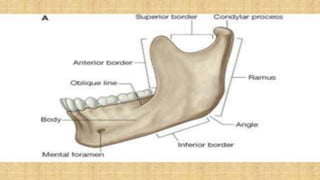
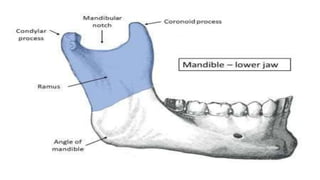
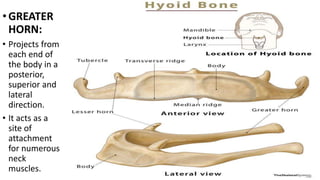
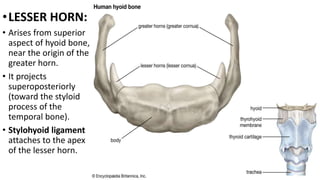
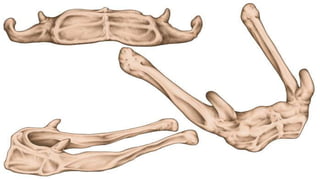
The document provides an overview of the mandible's anatomy, highlighting its structure, mobility, and various anatomical landmarks such as the body, ramus, and associated muscles. It also discusses clinical conditions related to the mandible, including fractures, cyst formation, and diseases such as osteomyelitis. Additionally, the document covers the anatomy and function of the hyoid bone and its relation to surrounding muscles and ligaments.

























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

