






![Cervical part
▪ Cervical part Runs upwards on superior constrictor of pharynx deep
to the posterior belly of digastric.
▪ It grooves the posterior border of sub-mandibular gland, makes S-
bend [2 loops] 1st winding down over sub-mandibular gland & then
up over the base of mandible.](https://image.slidesharecdn.com/thas-sem6-facialartery-200417060211/85/Facial-artery-32-320.jpg)
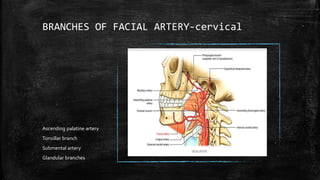
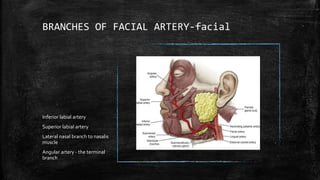



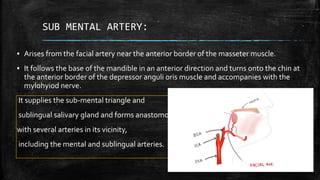






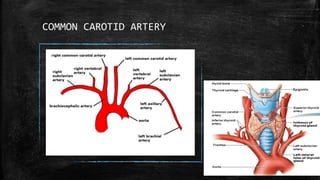
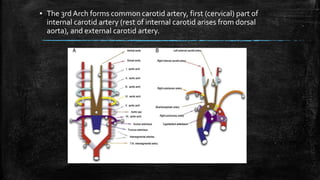
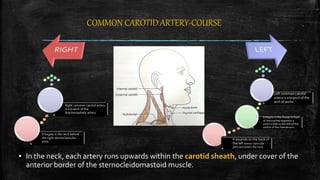
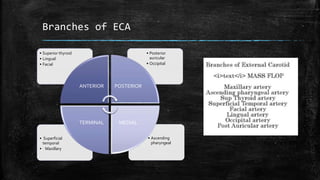
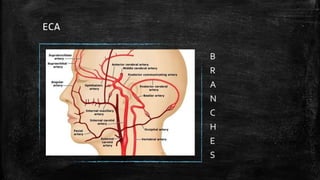
The document discusses the facial artery, which arises from the external carotid artery. It has both cervical and facial parts. The cervical part runs upwards in the neck, allowing movement of neck structures. It gives off branches like the ascending palatine and tonsillar arteries. The facial part enters the face by piercing the mandible. In the face, it gives branches like the inferior and superior labial arteries and terminates by anastomosing with the ophthalmic artery. The document also discusses the common carotid artery and its branches.
















































































