Downloaded 68 times


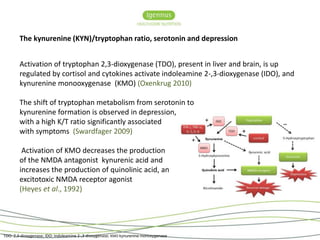
![AA to EPA ratio in health and disease
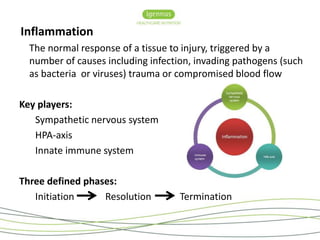
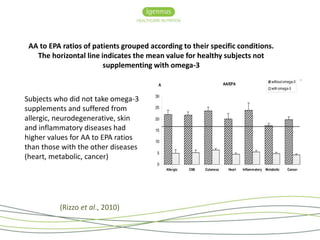
Fasted blood samples from 1432 [Italian] subjects, who were referred by
their physicians, were analysed to assess their AA to EPA and total omega-6 to
omega-3 ratios in whole blood and in RBC membrane phospholipids
Individuals with no diagnosable conditions had lower AA to EPA ratios than
those with diagnosable health conditions
Individuals with allergic, skin and neurodegenerative diseases had higher
ratios of AA to EPA compared to the values for subjects with other
pathologies, possibly due to a higher turnover of EPA
Subjects who did not take omega-3 supplements and suffered from allergic,
neurodegenerative, skin and inflammatory diseases had higher values for AA
to EPA ratios than those with the other diseases (heart, metabolic, cancer)
(Rizzo et al., 2010)](https://image.slidesharecdn.com/camexpotalk-141007101644-conversion-gate02/85/Managing-Chronic-Inflammation-24-320.jpg)
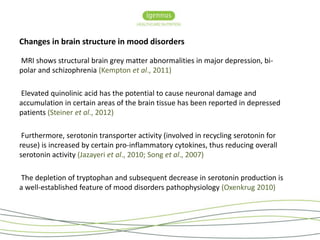
![AA to EPA ratio and the metabolic syndrome
High AA to EPA ratio associated with insulin resistance
Age and visceral fat accumulation correlated significantly with serum AA to
EPA ratio
Subjects with visceral fat accumulation ≥100 cm2 had higher serum AA to
EPA ratio (but not DHA to AA or [EPA+DHA] to AA) and more likely to have
metabolic syndrome and history of coronary artery disease, compared to
those with visceral fat accumulation <100 cm2 (Inoue et al., 2013)
“The balance of AA to EPA by lifestyle modification and medication (such as
EPA-based medications) could be useful in reducing the prevalence of the
metabolic syndrome and atherosclerosis” (Inoue et al., 2013)](https://image.slidesharecdn.com/camexpotalk-141007101644-conversion-gate02/85/Managing-Chronic-Inflammation-27-320.jpg)
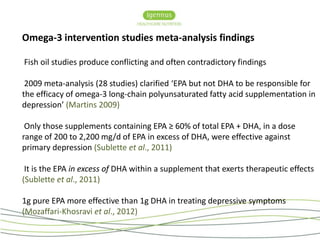
![High AA to EPA ratio and high levels of pro-inflammatory cytokines are directly
correlated with severity of depression, lower RBC membrane omega-3 and especially
EPA are associated with the severity of depression (Adams et al., 1996; Conklin et al.,
2007) and distinguish between anxious and non-anxious forms of major depressive
disorder (Liu et al., 2013)
Depression [in the elderly] is characterised by very low levels of omega-3, in
particular of EPA, in RBC membranes and a high AA to EPA ratio compared to healthy
subjects (Rizzo et al., 2012)
Omega-3 intervention lowers AA to EPA ratio and is correlated with improved scores
on the Geriatric Depression Scale (GDS) (Rizzo et al., 2012)
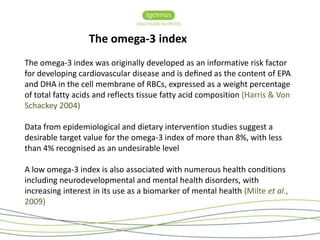
Omega-3 Index (mean, 3.9% vs 5.1%) and individual omega-3 fatty acids were
significantly lower in major depressive disorder patients. An Omega-3 Index < 4%
was associated with high concentrations IL-6 (indicative of an elevated cardiovascular
risk profile (Baghai et al., 2011)](https://image.slidesharecdn.com/camexpotalk-141007101644-conversion-gate02/85/Managing-Chronic-Inflammation-45-320.jpg)
![Summary
Western dietary and lifestyle factors, particularly those that create an
inflammatory environment, contribute significantly to inflammatory related
disorders
Diets that are high in omega-6 increase ‘risk’, whilst diets that are rich in long-chain
omega-3 may reduce the ‘risk’
Specifically, a high AA to EPA ratio and low EPA [rather than DHA] appears to
be associated with many inflammatory conditions
Modifying the diet can reduce systemic inflammation by manipulating the AA
to EPA ratio](https://image.slidesharecdn.com/camexpotalk-141007101644-conversion-gate02/85/Managing-Chronic-Inflammation-52-320.jpg)
![Summary
Human intervention studies show inconsistent findings – is there a need
for personalising omega-3 fatty acid dosing for clinical outcomes?
Not all ‘fish oils’ are the same – acknowledge the significance of the EPA to
DHA ratio
Pure EPA is a safe adjunctive therapy for inflammatory disorders
Evidence suggests that the presence of DHA within the therapeutic oil may
be [in some conditions] undesirable
Pure EPA, because of its safety and known anti-cancer benefits, is now
entering phase III human trials as a chemopreventive agent
Pure EPA is recognised for its cardiovascular health benefits](https://image.slidesharecdn.com/camexpotalk-141007101644-conversion-gate02/85/Managing-Chronic-Inflammation-53-320.jpg)


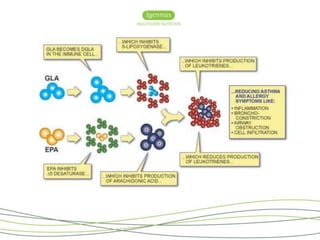

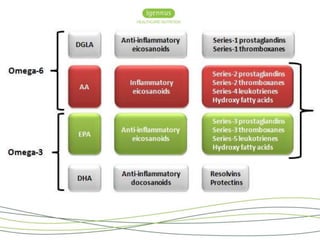
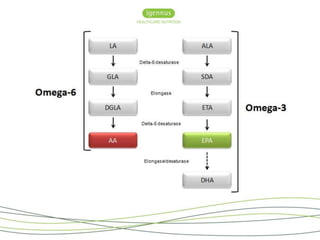
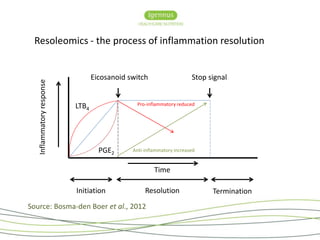
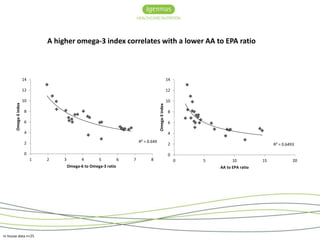
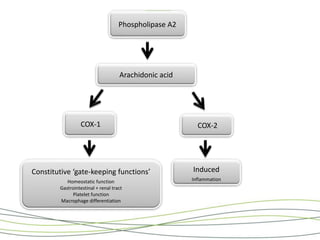
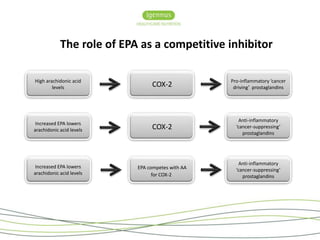
This document summarizes a presentation on managing chronic inflammation through modulating fatty acids like omega-3 and arachidonic acid. It discusses how inflammation contributes to diseases like cancer and dementia, and how biomarkers like the omega-3 index, omega-6/omega-3 ratio, and AA/EPA ratio can be used to personalize omega-3 dosing to reduce inflammation. Clinical evidence suggests EPA in particular may help treat inflammation and inhibit cancer progression by competing with arachidonic acid metabolism.























































































