Downloaded 122 times
















![Fibromyalgia and cytokines
FMS isn’t generally classified as an autoimmune disease per se, but it shares many traits with
autoimmune-like diseases in which the body is attacking itself, often as a result of chronic
overproduction of inflammatory cytokines
•Features found in FMS (elevated numbers of B cells and cytokines and decreased numbers of
T regulatory [Treg] cells) are associated commonly with autoimmune diseases
•Cytokines have effects on the HPA-axis, the sympathetic nervous system and T lymphocytes,
which in turn might be associated with fibromyalgia
•Studies of cytokine levels in patients with fibromyalgia suggest that levels of the
proinflammatory cytokines IL-1, IL-6 and IL-8 are elevated, whereas TNFα levels are normal,
and levels of the antiinflammatory cytokines IL-4 and IL-10 are unchanged or reduced
•Treg are responsible for turning inflammation on and off and can help prevent an immune
system from becoming overactive and eventually leading to autoimmune dysfunction
•The % of Treg that suppresses the immune response appear to be reduced in a number of
stress-related diseases/conditions
https://igennus.com/practitioner-blog/nutrition-interventions-adhd-focus-treg/
Wallace DJ, Linker-Israeli M, Hallegua D, Silverman S, Silver D, Weisman MH. Cytokines play an aetiopathogenetic role in fibromyalgia: a hypothesis and pilot study. Rheumatology
(Oxford). 2001 Jul;40(7):743-9.
Generaal, E. et al. Basal inflammation and innate immune response in chronic multisite musculoskeletal pain. Pain 155, 1605–1612 (2014).](https://image.slidesharecdn.com/fibromyalgiawebinar-171201153428/85/Fibromyalgia-a-clinical-approach-18-320.jpg)

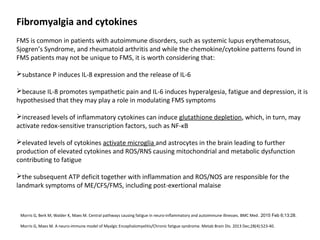




































![Serving size: 2 tablets Per serving %Reference Intake
Vitamin C (ascorbic acid) 240 mg 300
Vitamin B3 (nicotinamide) 48 mg NE 300
Zinc citrate 20 mg 200
Vitamin B5 (pantothenic acid) 18 mg 300
Vitamin B6 (pyridoxal 5-phosphate) 8 mg 570
Iron (ferrous bisglycinate chelate) 7 mg 50
Vitamin B1 (thiamine HCl) 5.5 mg 500
Vitamin B2 (riboflavin 5-phosphate) 4.2 mg 300
Vitamin E D-alpha tocopherol (natural) 2 mg a-TE 16.6
Boron (disodium tetraborate) 2 mg n/a
Manganese bisglycinate 2 mg 100
Copper bisglycinate 1 mg 100
Vitamin A (beta carotene) 800 mg 100
Folate ([6S]-5-methyltetrahydrofolate) 200 mg 100
Selenomethionine 110 mg 200
Iodine (kelp) 150 mg 100
Vitamin B7 (biotin) 100 mg 200
Chromium picolinate 50 mg 125
Molybdenum 50 mg 100
Vitamin K2 (menaquinone) 37.5 mg 50
Vitamin B12 (methylcobalamin) 20 mg 800
Vitamin D3 (cholecalciferol) 10 mg (400 iu) 200
MULTIVITAMIN & MINERALS™
provides 22 key essential vitamins &
minerals in superior body-ready and
active forms for enhanced absorption
and utilisation.
Our sustained slow release system
optimises blood nutrient levels for
longer-lasting action.](https://image.slidesharecdn.com/fibromyalgiawebinar-171201153428/85/Fibromyalgia-a-clinical-approach-57-320.jpg)

![MindCare LIFT
Nutritional information Per capsule % reference
intake
Magnesium glycinate
of which magnesium
334 mg
60 mg 16
5-HTP 100 mg n/a
Vitamin B3 (niacin) 48 mg 300
Vitamin C (ascorbic acid) 40 mg 50
Zinc (citrate) 20 mg 200
Vitamin B5 (pantothenic acid) 12 mg 200
Vitamin B6
(pyridoxal-5-phosphate)
7.98 mg 570
Vitamin B1 (thiamine) 3.3 mg 300
Vitamin B2 (riboflavin) 2.8 mg 200
Vitamin B7 (biotin) 150 mg 300
Folate
([6S]-5-methyltetrahydrofolate)
100 mg 50
Selenium 82.5 mg 150
Vitamin B12 (methylcobalamin) 20 mg 800
Nutritional information Per capsule % reference
intake
Omega-3 rTG concentrated fish oil
of which:
EPA (eicosapentaenoic acid)
DHA (docosahexaenoic acid)
893 mg
410 mg
250 mg
n/a
Vitamin E (d-alpha tocopherol) 6mg 50
Vitamin D3 25 mg 500](https://image.slidesharecdn.com/fibromyalgiawebinar-171201153428/85/Fibromyalgia-a-clinical-approach-59-320.jpg)


Fibromyalgia syndrome (FMS) is a chronic pain condition primarily affecting women aged 25 to 55, characterized by widespread pain, fatigue, and diverse somatic symptoms. Diagnosis is based on specific criteria involving pain index scores and symptom severity, with potential genetic and environmental risk factors contributing to its onset. Abnormal levels of cytokines, neurotransmitters, and hormonal imbalances may also be involved in the disease's pathogenesis, leading to overlapping conditions and heightened pain sensitivity.























































































