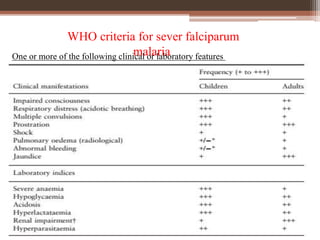
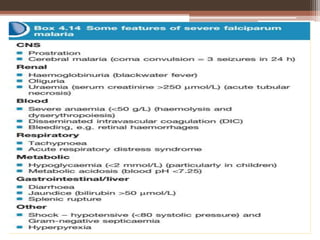
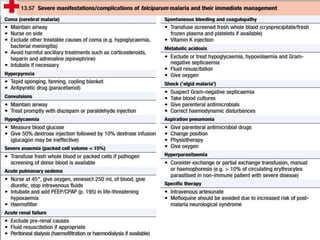
Malaria is caused by Plasmodium parasites, with P. falciparum being the most deadly. Clinical features of malaria include flu-like symptoms such as fever, fatigue, and muscle aches. Fever occurs in periodic paroxysms, with shivering, high fever, and sweating stages. Complications of severe falciparum malaria include cerebral malaria, hypoglycemia, acidosis, anemia, disseminated intravascular coagulation, liver dysfunction, pulmonary edema, and renal impairment. Cerebral malaria is the most important complication and a leading cause of death from malaria.