Downloaded 76 times

Plasmodium falciparum malaria poses a serious global health threat, with approximately 250 million cases and 1 million deaths annually. Drug resistance has developed to former first-line treatments such as chloroquine and sulfadoxine-pyrimethamine. Prompt diagnosis and treatment with artemisinin-based combination therapies can reduce the spread of resistance. A malaria vaccine is still in development but one candidate, RTS,S, has shown promise in clinical trials in reducing malaria cases and severity.
Introduction to Plasmodium falciparum and its association with multi-drug resistant malaria. Presented by Vani Vannappagari at the 41st Annual Symposium.
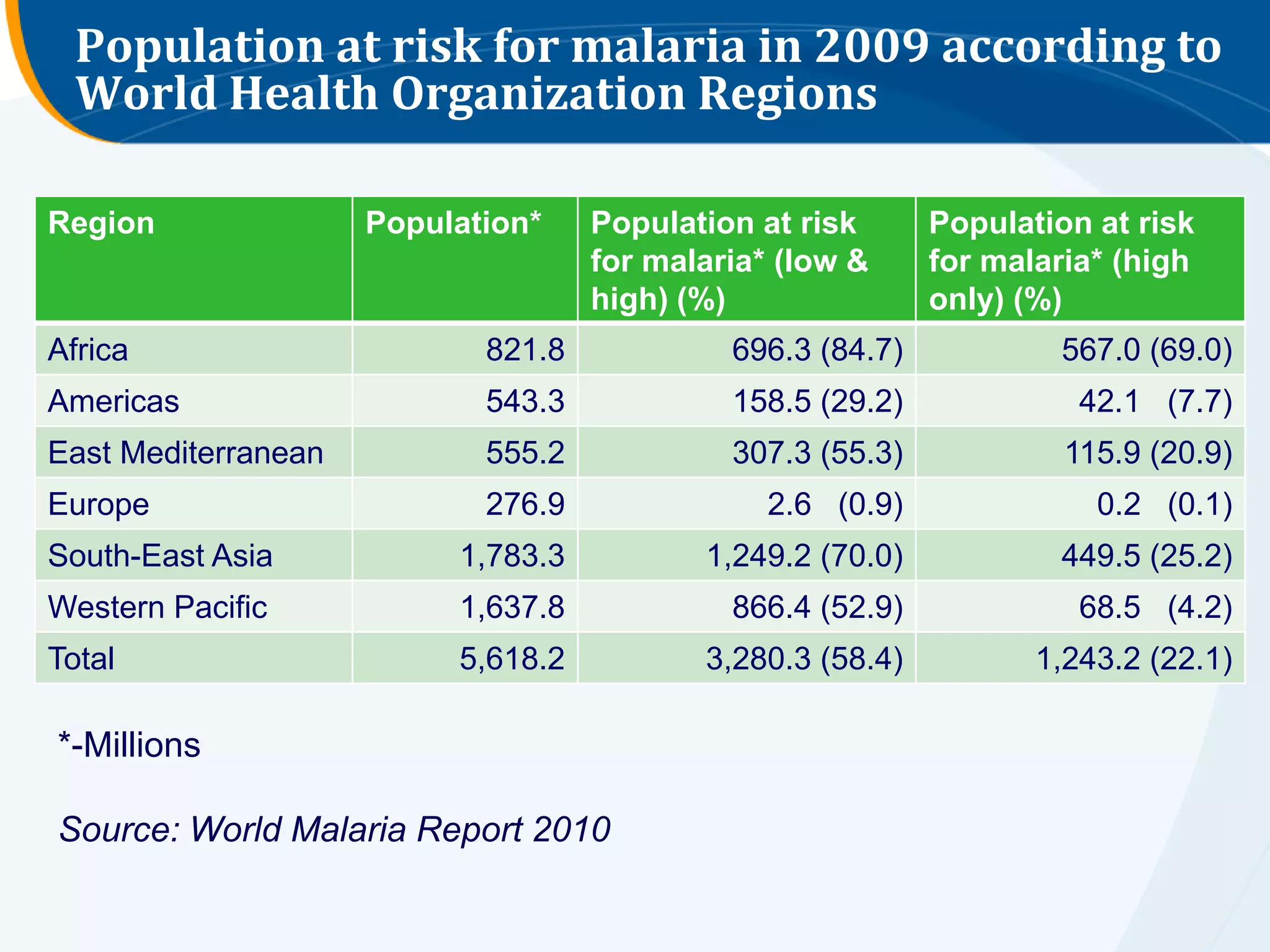
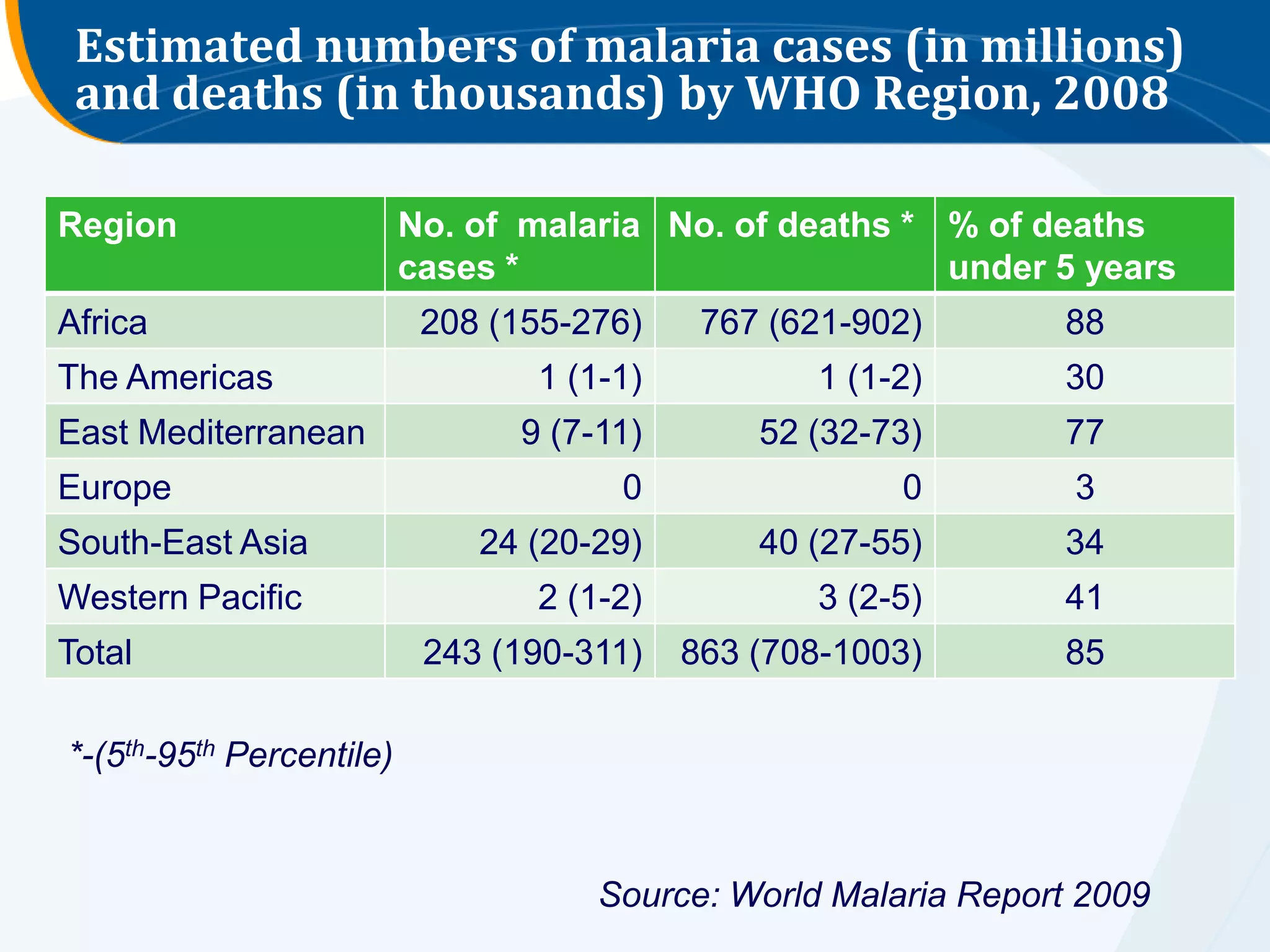
Malaria cases: ~250 million and ~1 million deaths annually, with 85%<5 years old. 3.2 billion at risk.
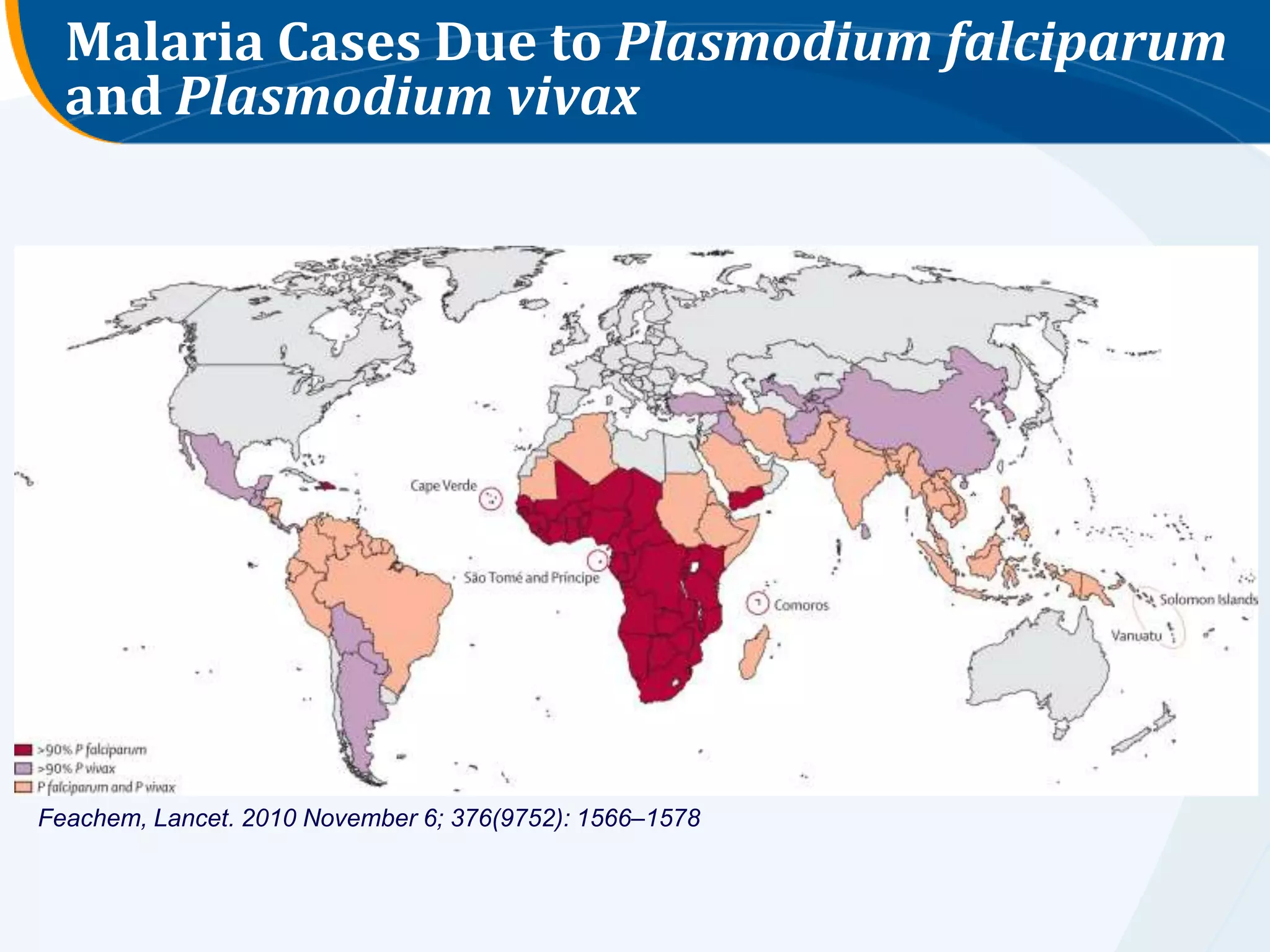
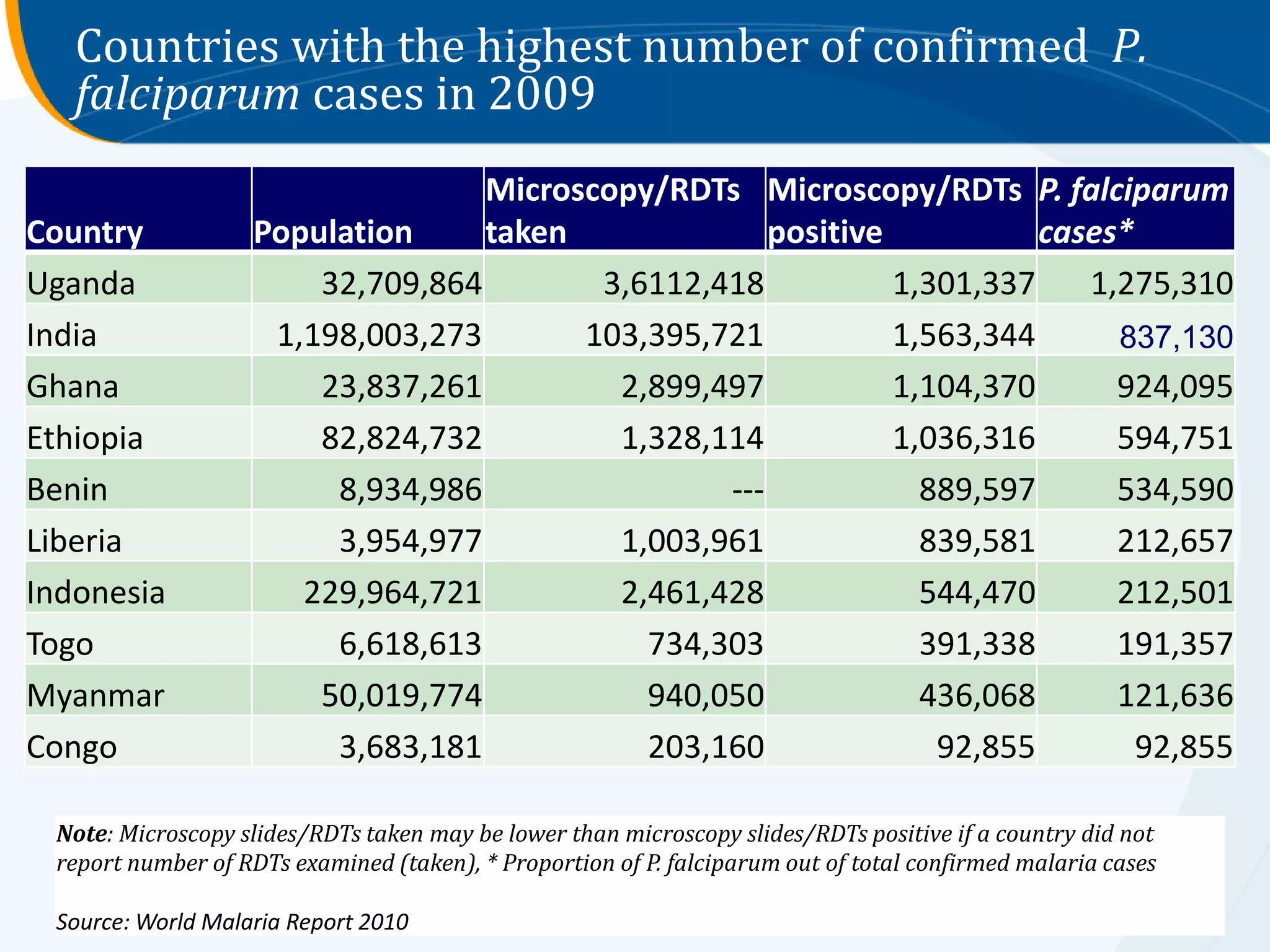
Five Plasmodium species infect humans. P. falciparum accounts for >75% of cases and deaths in SSA.
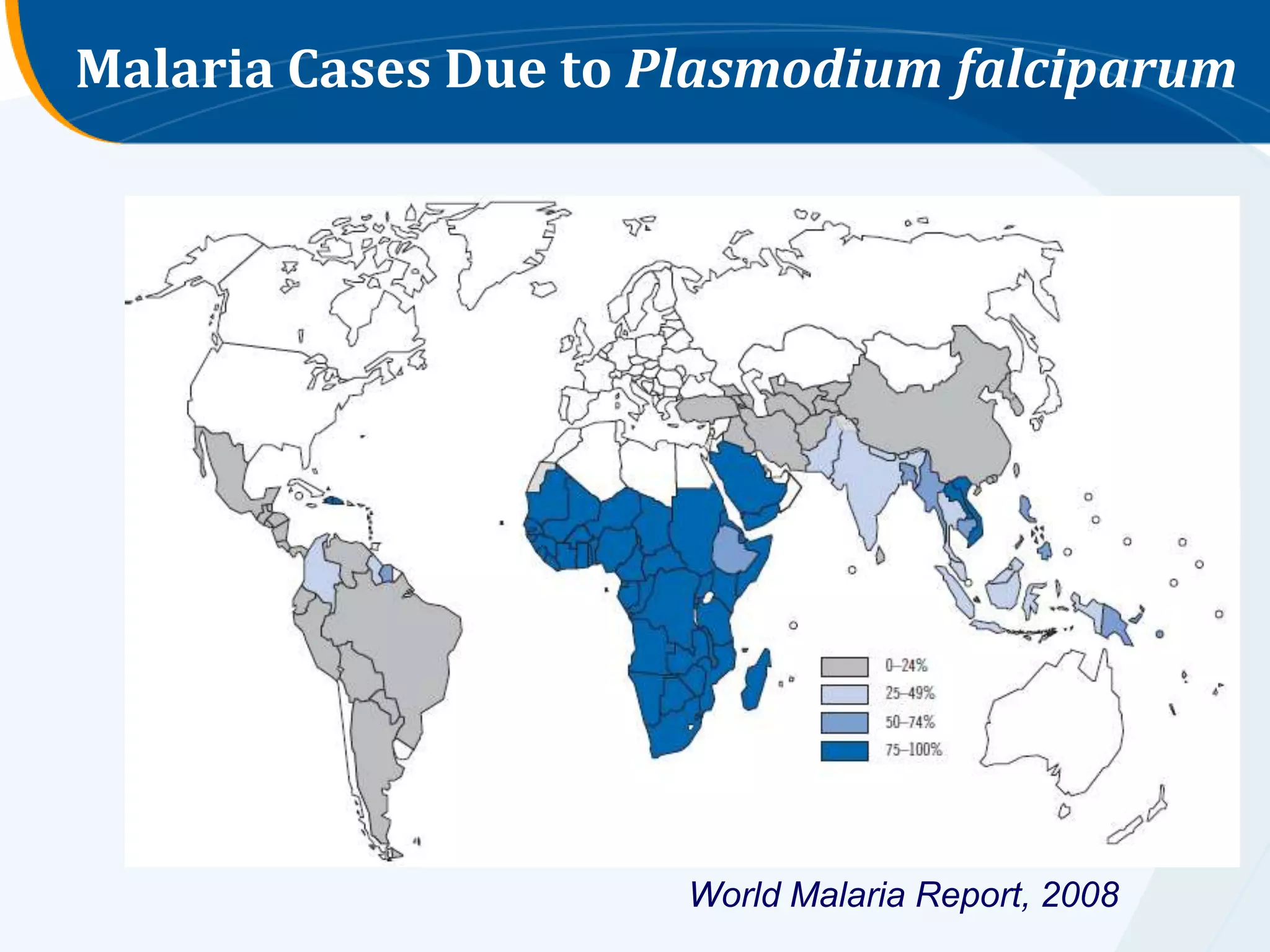
Data on malaria cases due to P. falciparum from World Malaria Report 2008 and supplementary Lancet data.
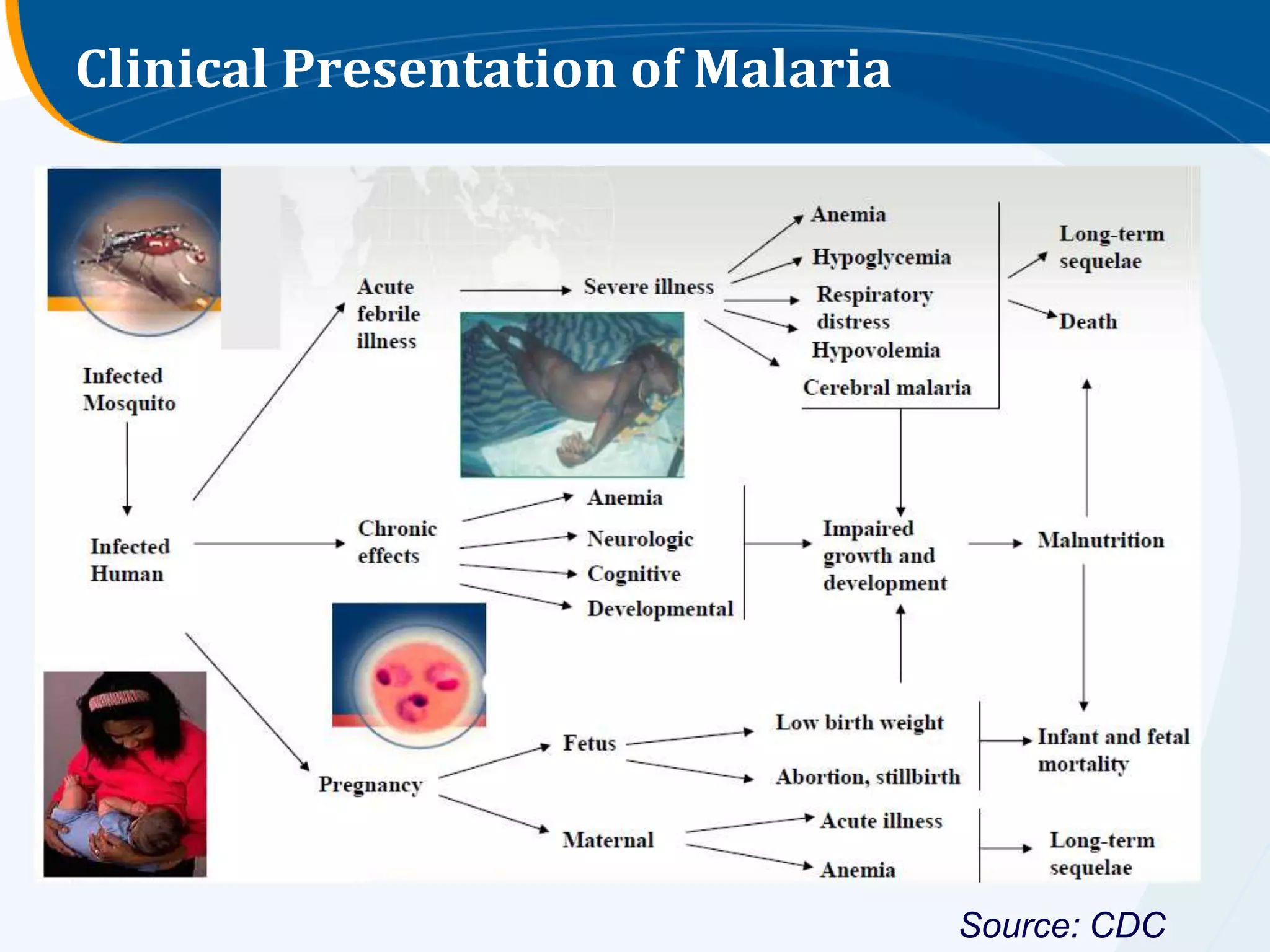
Overview of malaria symptoms, aiding diagnosis.
Diagnosis through clinical methods, microscopy as gold standard, and various testing methods discussed.
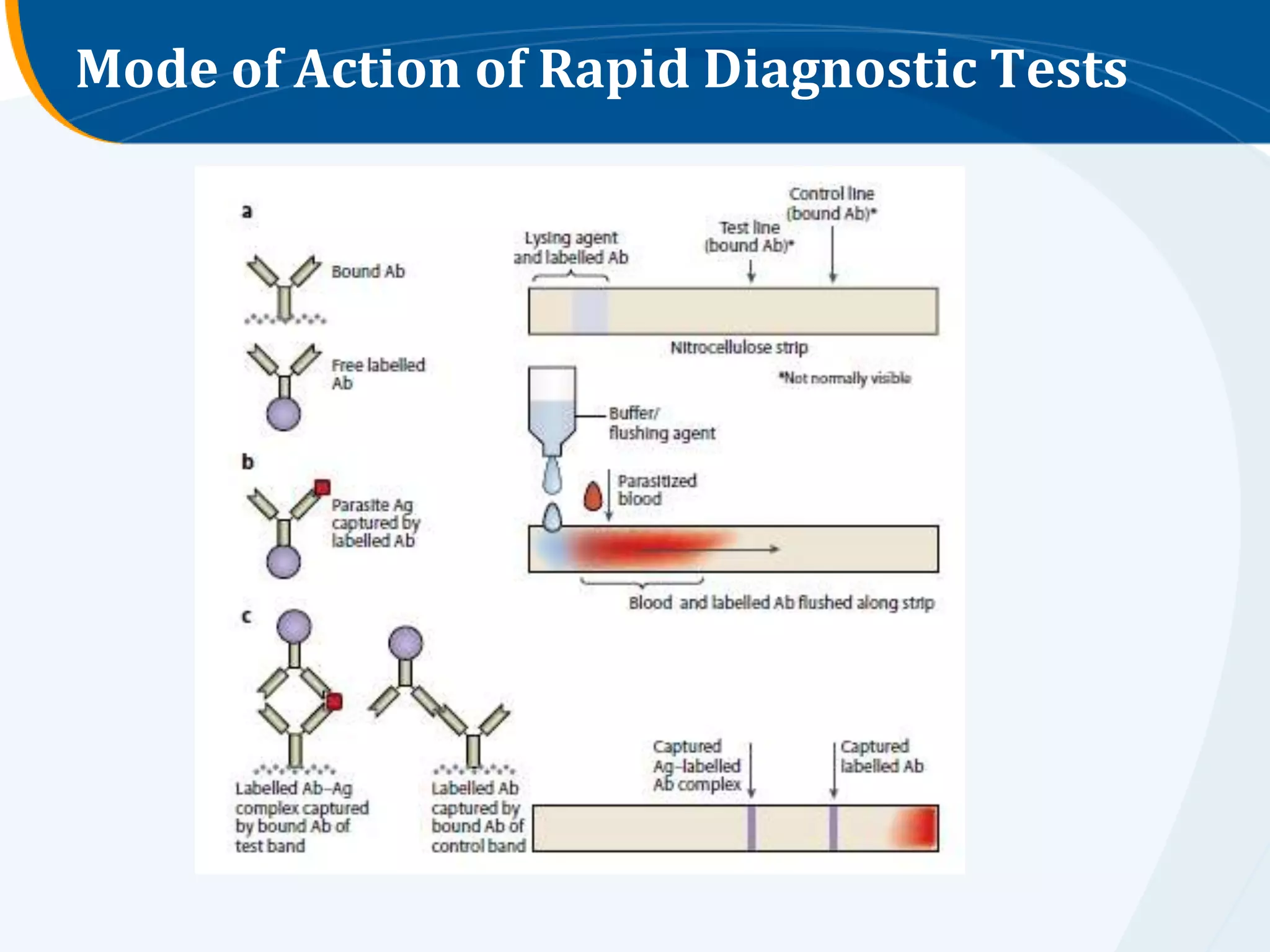
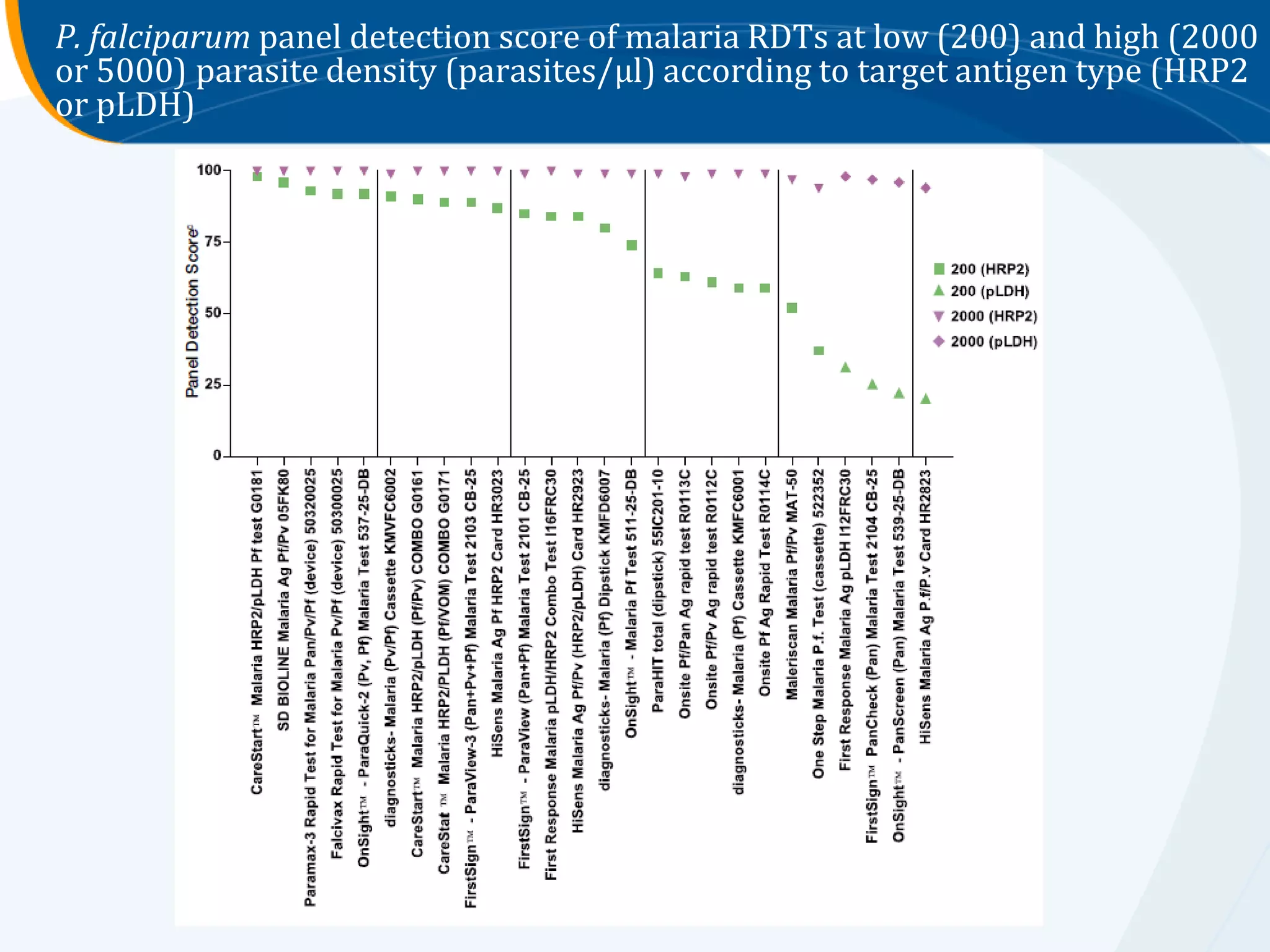
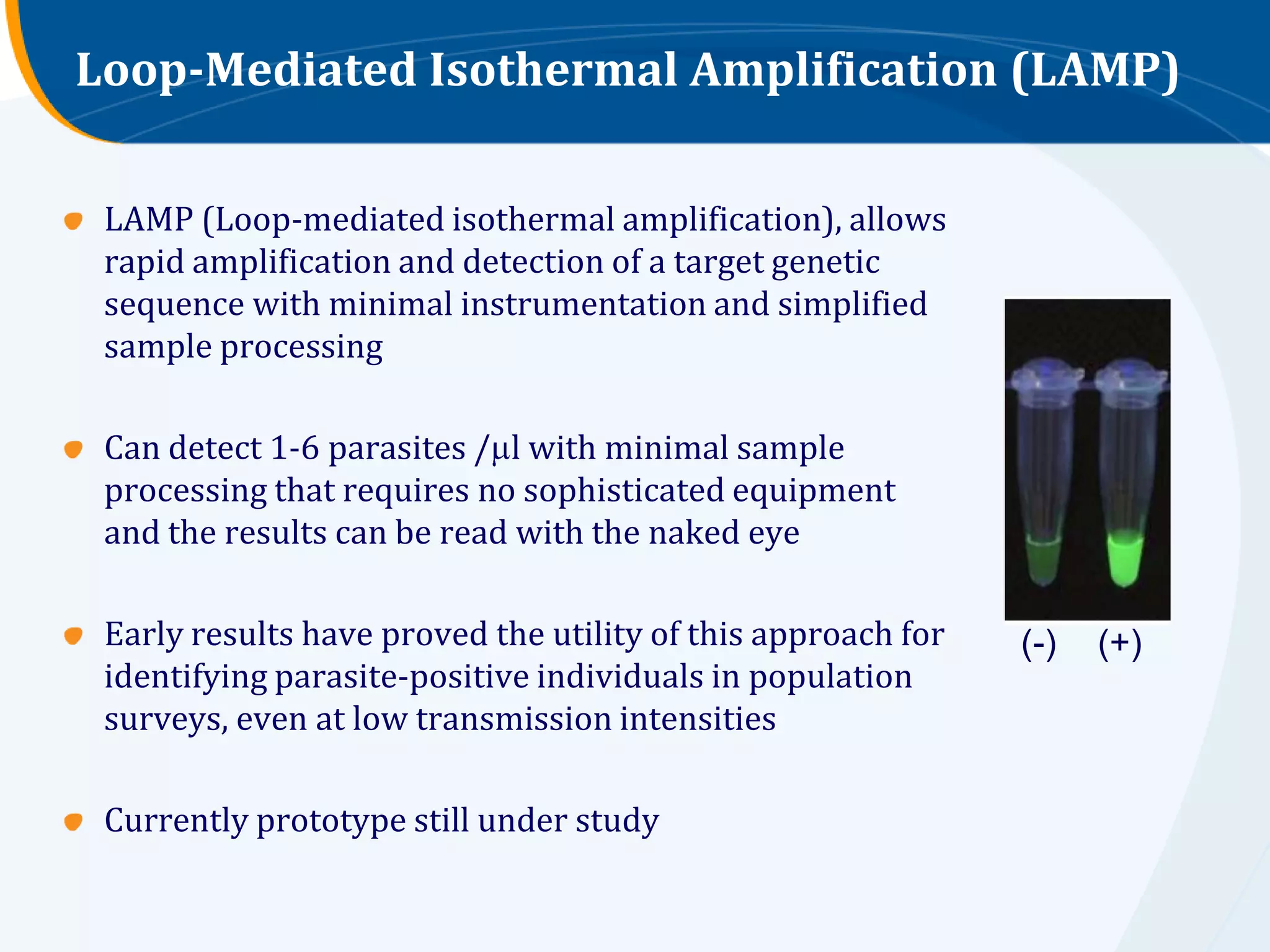
Details of various advanced diagnostic tests including rapid tests, PCR methods, and NALFIA.
Statistics on clinical diagnosis usage globally, highlighting issues with confirmation rates before treatment.
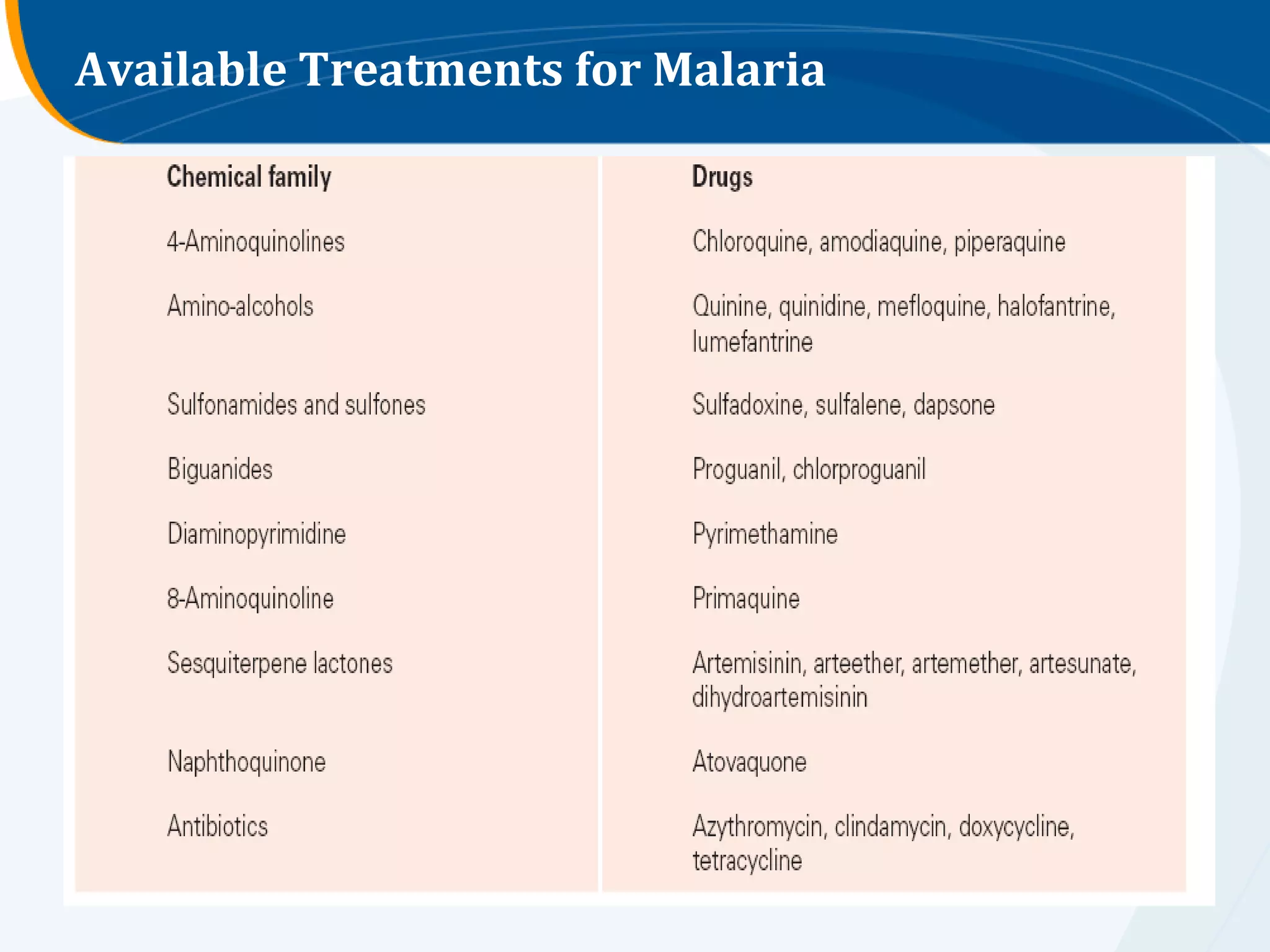
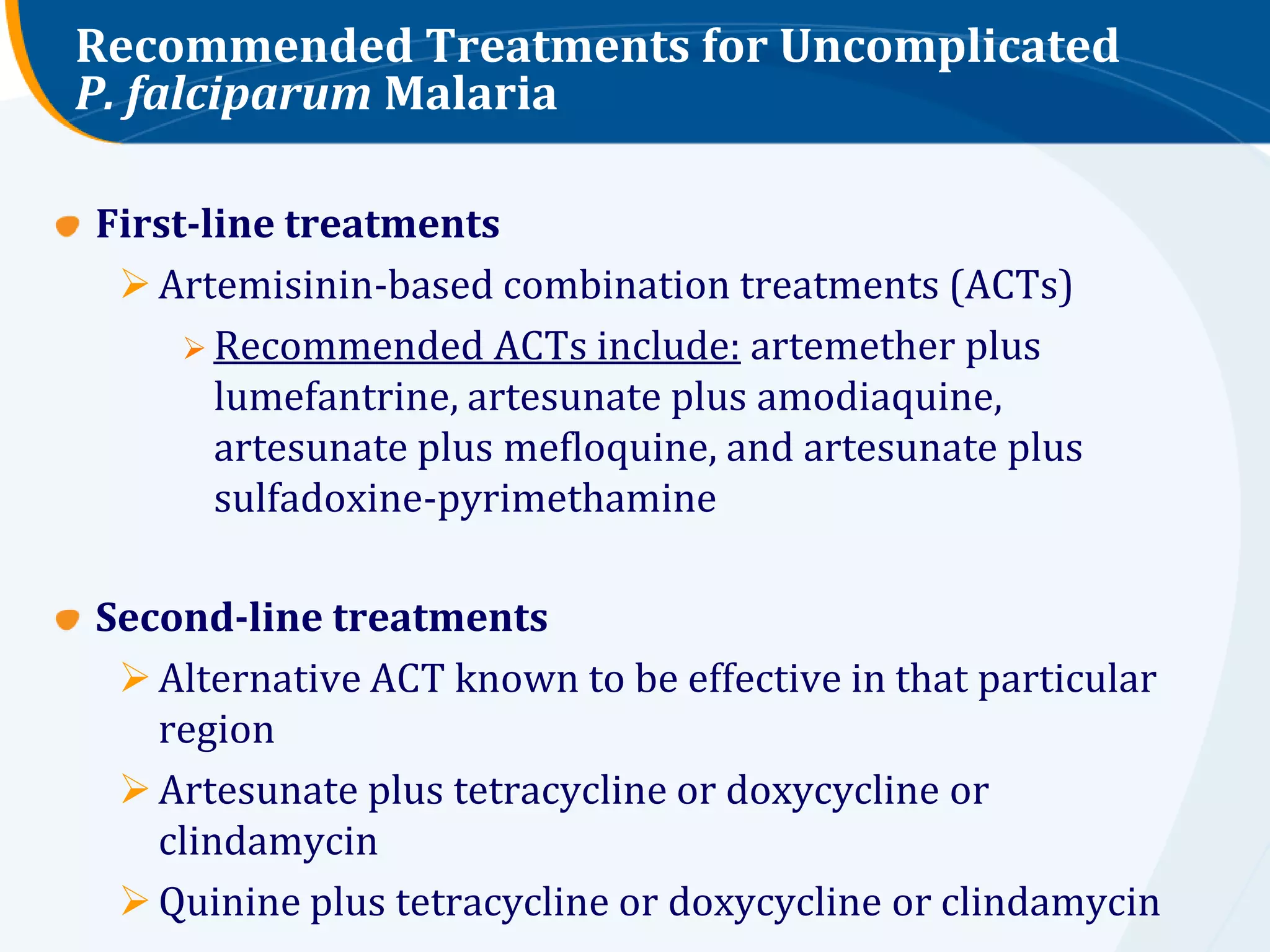
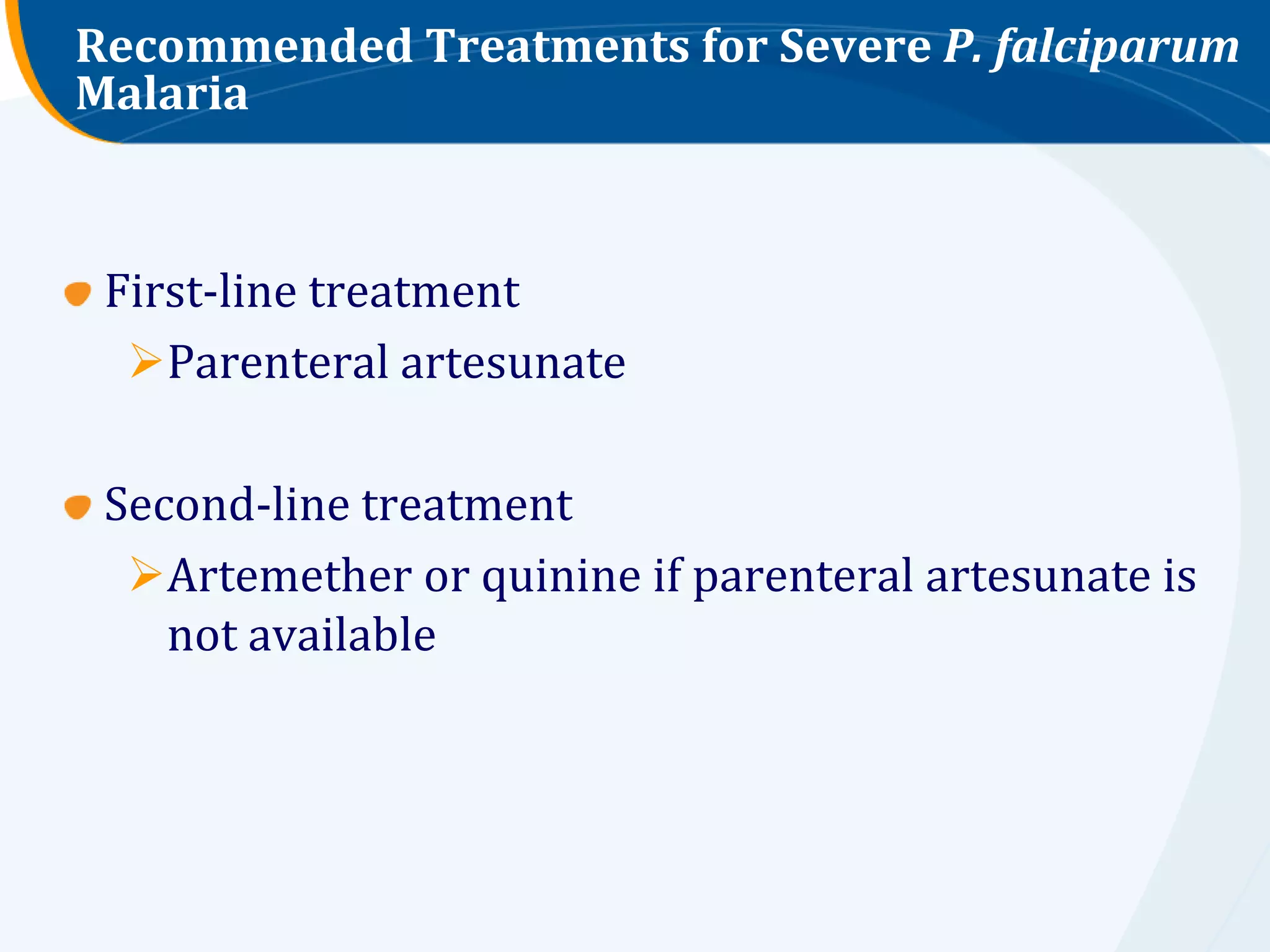
Overview and guidelines for treating uncomplicated and severe P. falciparum malaria.
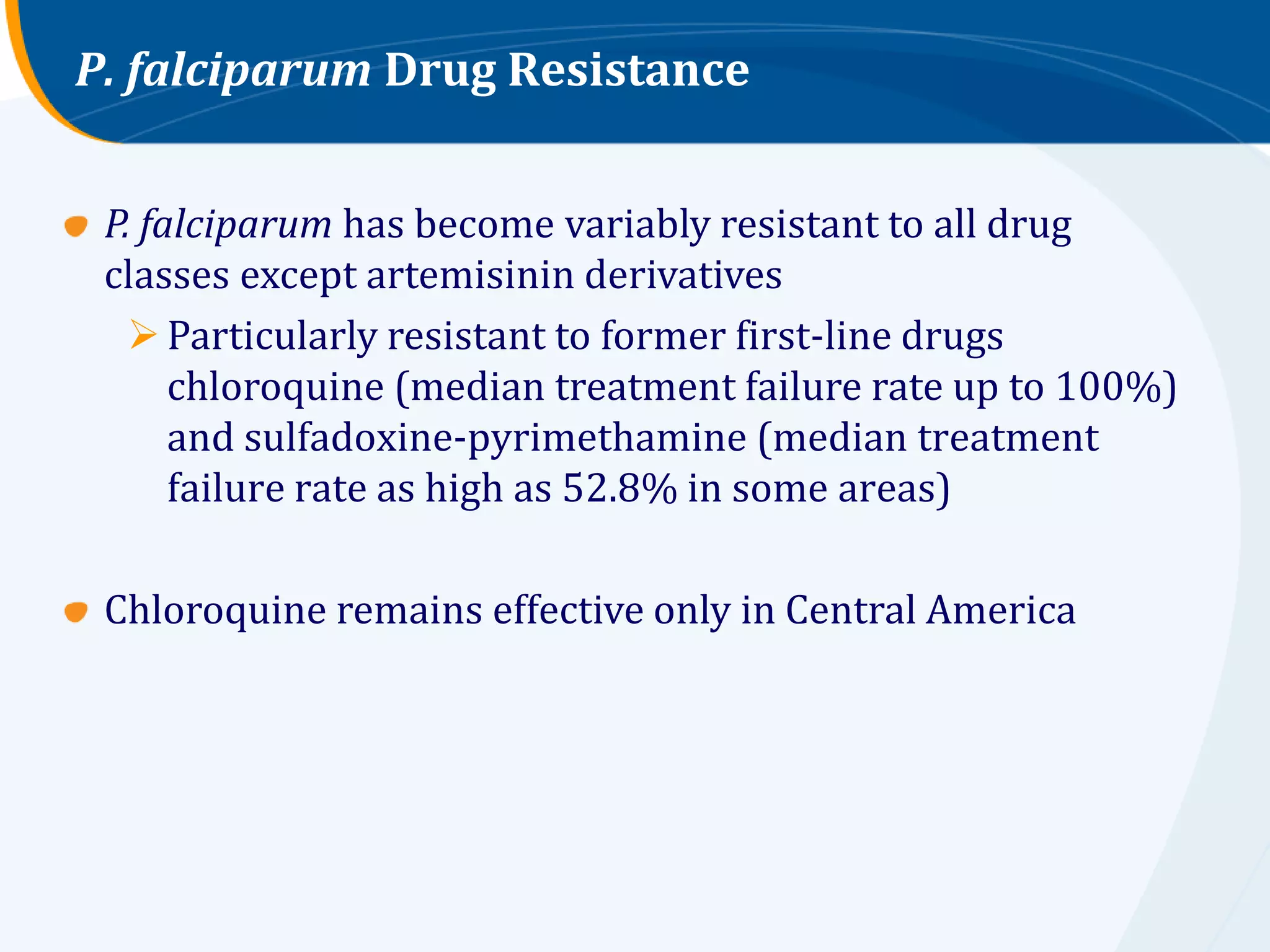
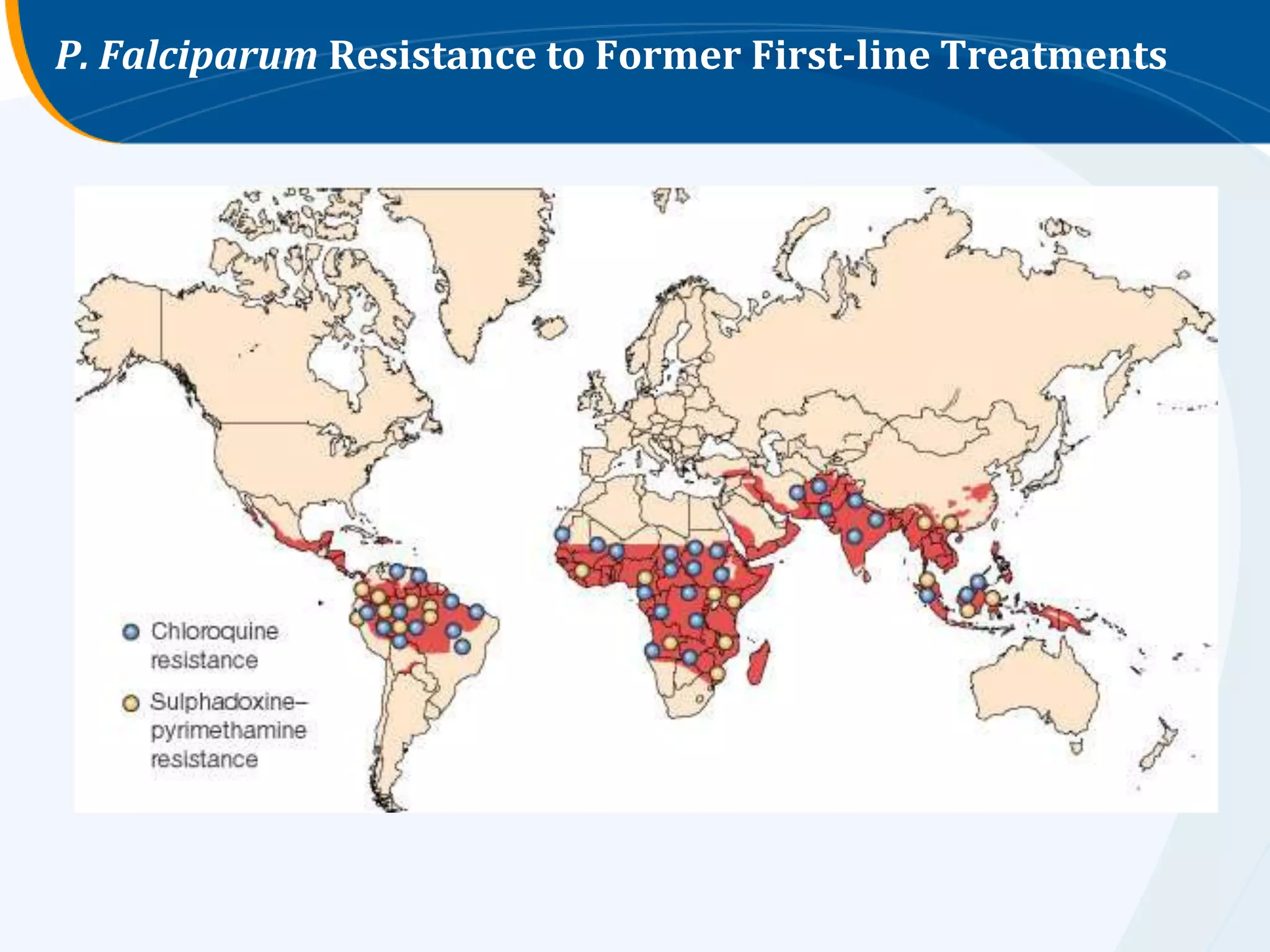
Rising resistance of P. falciparum to drugs, notably chloroquine and sulfadoxine-pyrimethamine.
Uncontrolled drug use, poor drug quality, and sub-therapeutic levels contributing to resistance.
Strategies for delaying resistance spread: early diagnosis, insect control, and disease monitoring.
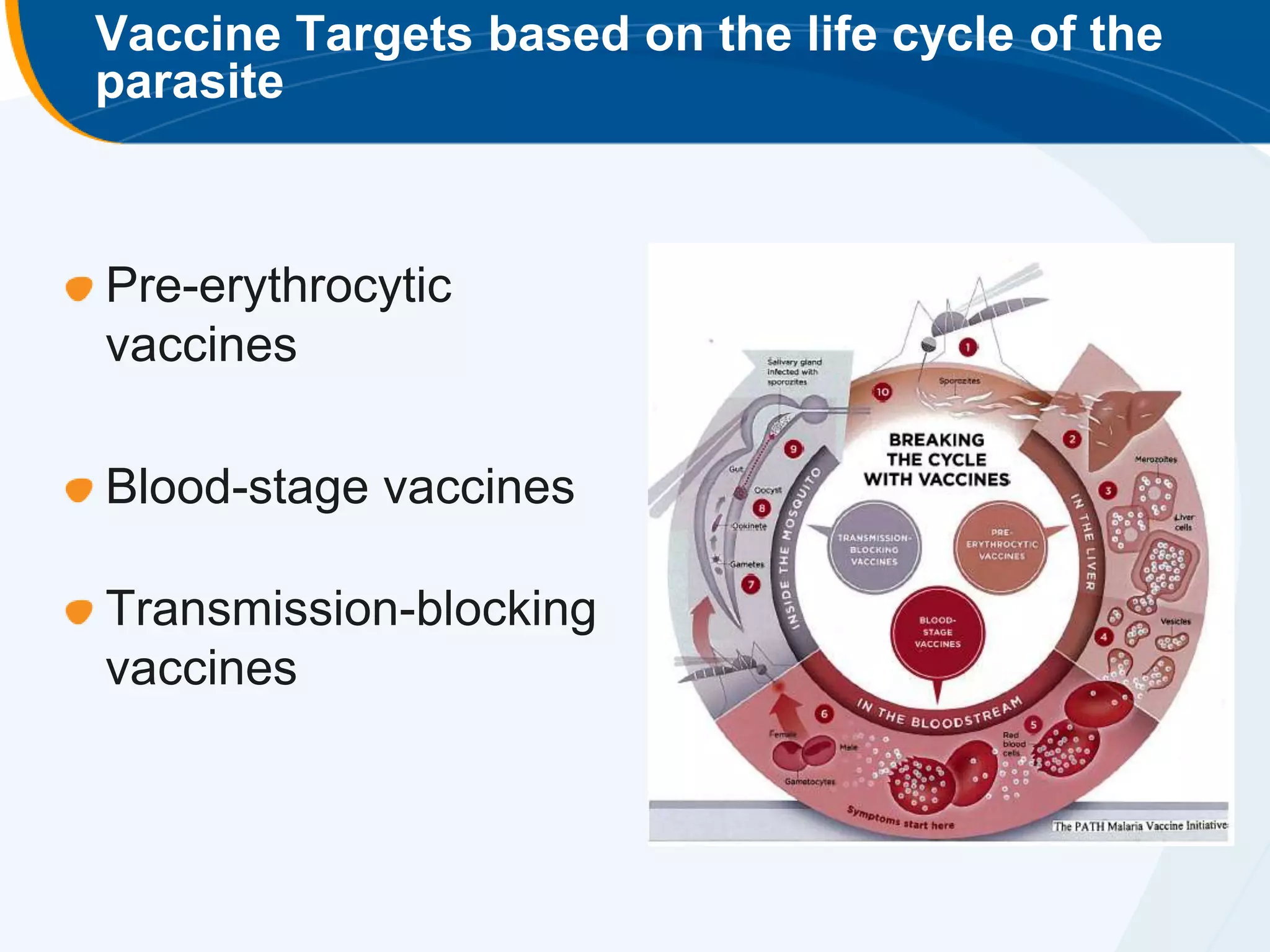
Types of malaria vaccines being developed: pre-erythrocytic, blood-stage, and transmission-blocking.
Most advanced vaccine candidate: RTS,S showing efficacy in trials against clinical malaria.
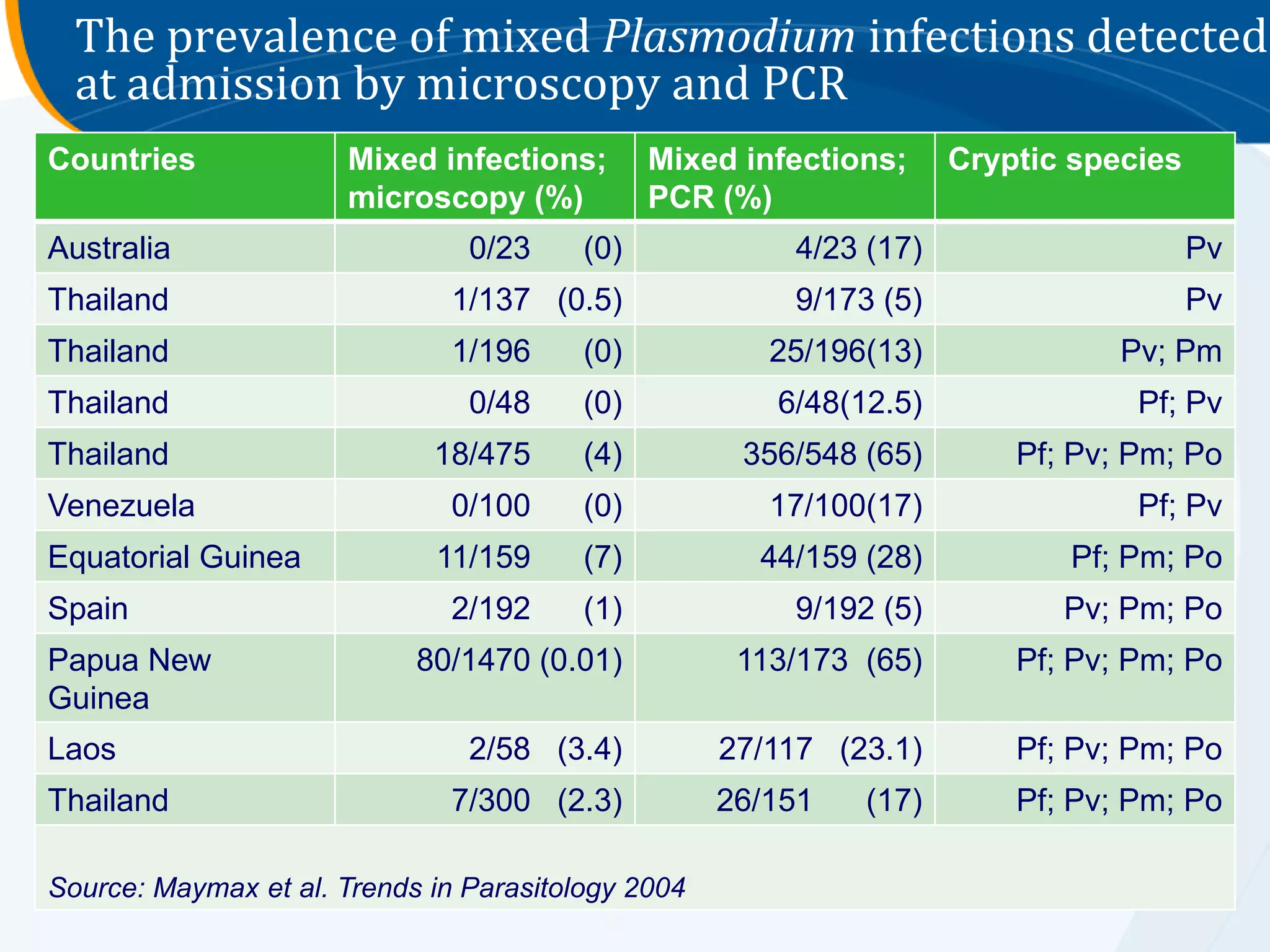
Statistics on malaria populations at risk, estimated cases, deaths by WHO region, and mixed infections.
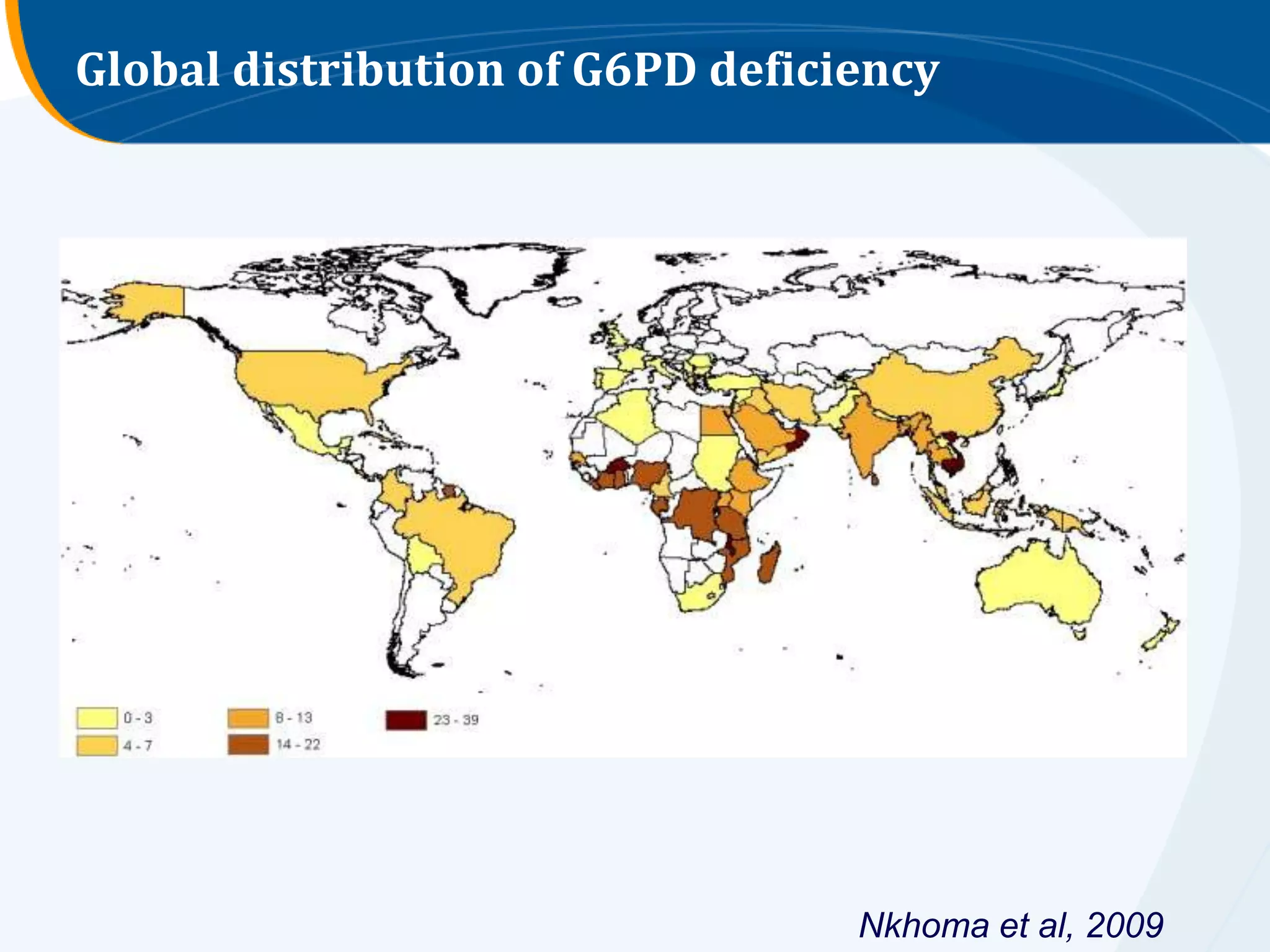
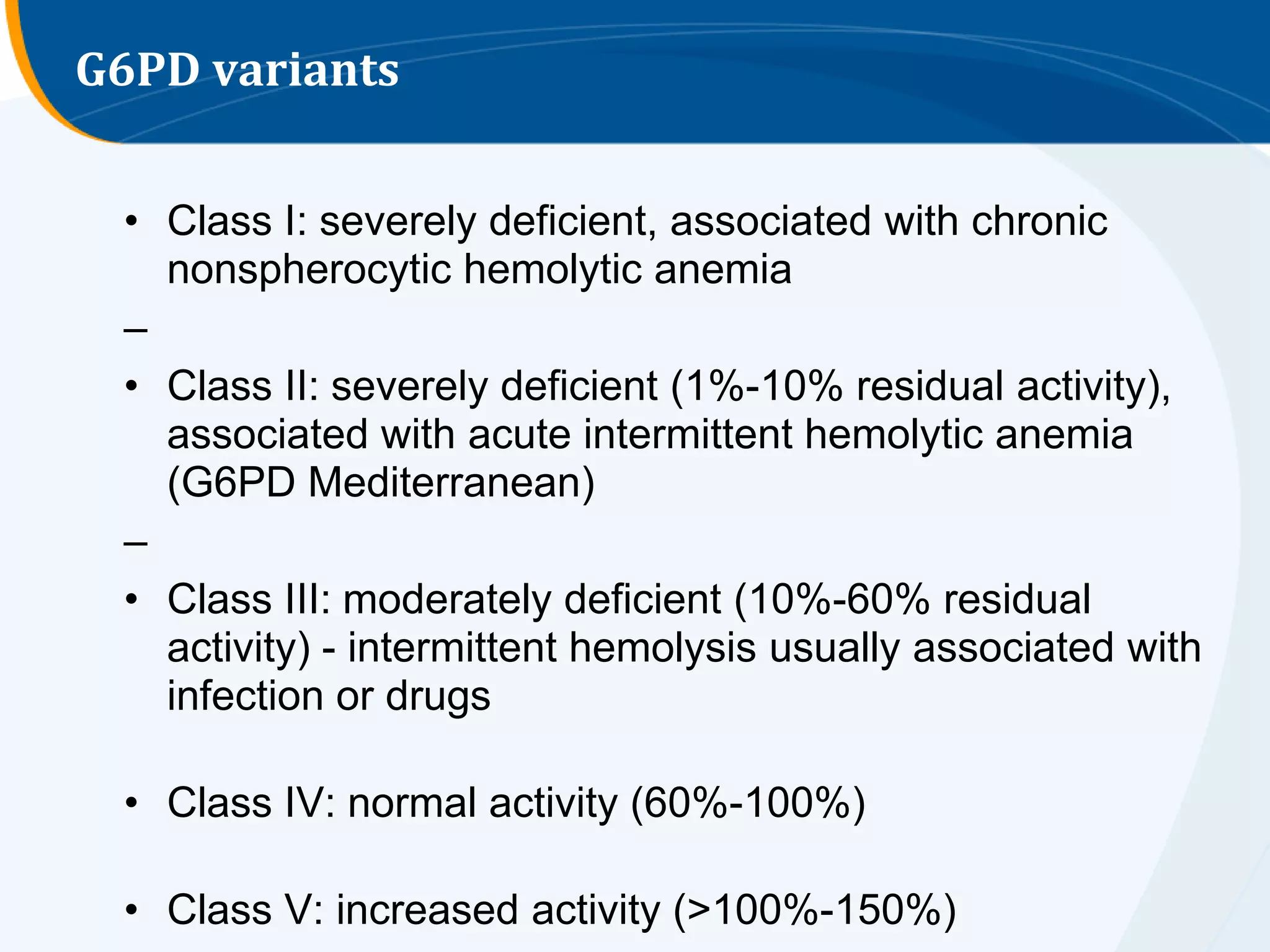
Overview of G6PD deficiency impact on malaria, detailing its global prevalence and variant classifications.
Objectives for treating malaria: prevent severe disease, drug resistance, and reduce transmission.
Guidelines for treating various demographics, including special populations like pregnant women and infants.





















































































![Rheumatic Fever CASE PRESENTATION [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationautosaved-251123182512-9d9b0da4-thumbnail.jpg?width=640&height=640&fit=bounds)
