Downloaded 60 times














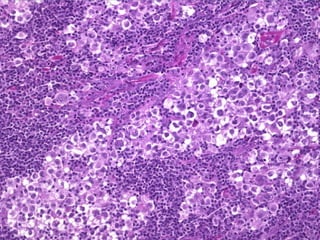











This document discusses different types of lymphoid neoplasms, or cancers affecting the lymphatic system. It describes non-Hodgkin's lymphomas like chronic lymphocytic leukemia, MALT lymphoma, and follicular lymphoma. It also discusses Hodgkin's lymphoma and its subtypes of lymphocyte rich, nodular sclerosis, mixed cellularity, and lymphocyte depletion. Specific lymphomas mentioned include acute lymphoblastic leukemia, diffuse large B-cell lymphoma, and Burkitt's lymphoma.











































































































