Downloaded 161 times
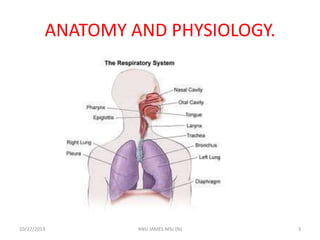
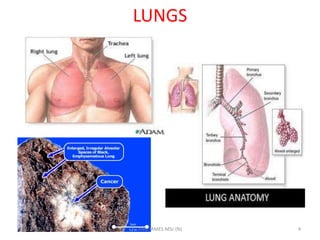
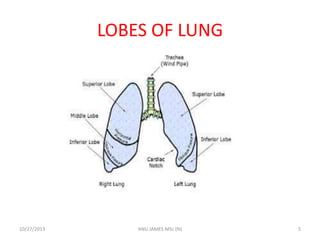
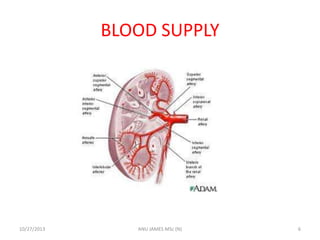


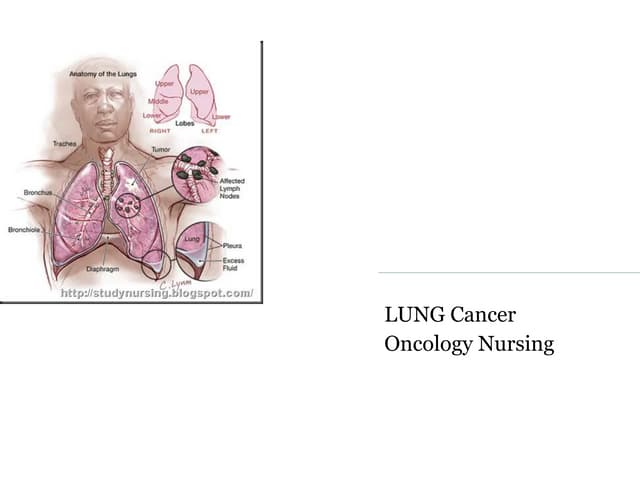
The document presents information about lung cancer presented by Anu James. It defines lung cancer, describes the anatomy and physiology of the lungs, and discusses the etiology, risk factors, types, pathophysiology, clinical manifestations, diagnostic evaluations, management including medical, radiation and surgical options, nursing management, complications, and health education related to lung cancer.