Downloaded 4,123 times
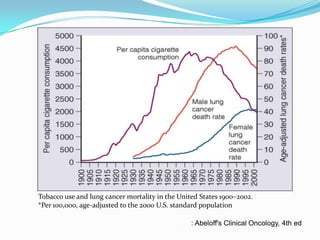
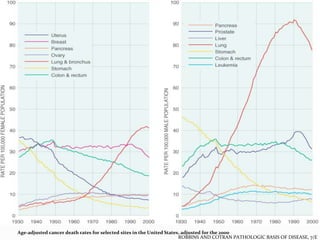
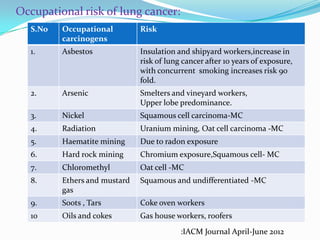
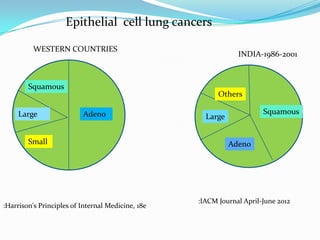
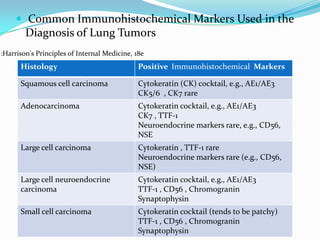
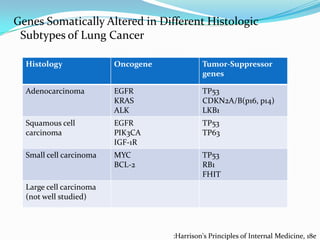

This document discusses lung cancer epidemiology, risk factors, pathology, and smoking cessation. It notes that lung cancer is largely caused by tobacco consumption and was rare before the 20th century. While smoking is the primary risk factor, some people who develop lung cancer have never smoked. The four main histological types are small cell lung cancer, adenocarcinoma, squamous cell carcinoma, and large cell carcinoma. Stopping smoking can avoid over 90% of lung cancer risk from tobacco. Occupational exposures like asbestos and radiation also increase lung cancer risk.














































































