Downloaded 27 times

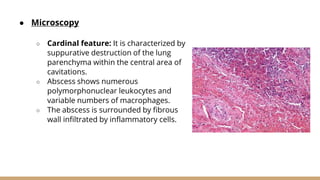
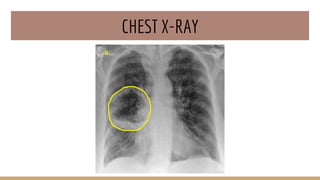


Lung abscess is a localized suppurative process marked by pus accumulation and lung tissue destruction, classified as acute or chronic and primary or secondary based on etiology. Common causative organisms are anaerobic and aerobic bacteria, with clinical features including foul-smelling sputum, fever, and weight loss. Diagnosis involves history taking, imaging, and cultures, while management includes antibiotics and possible surgical intervention.