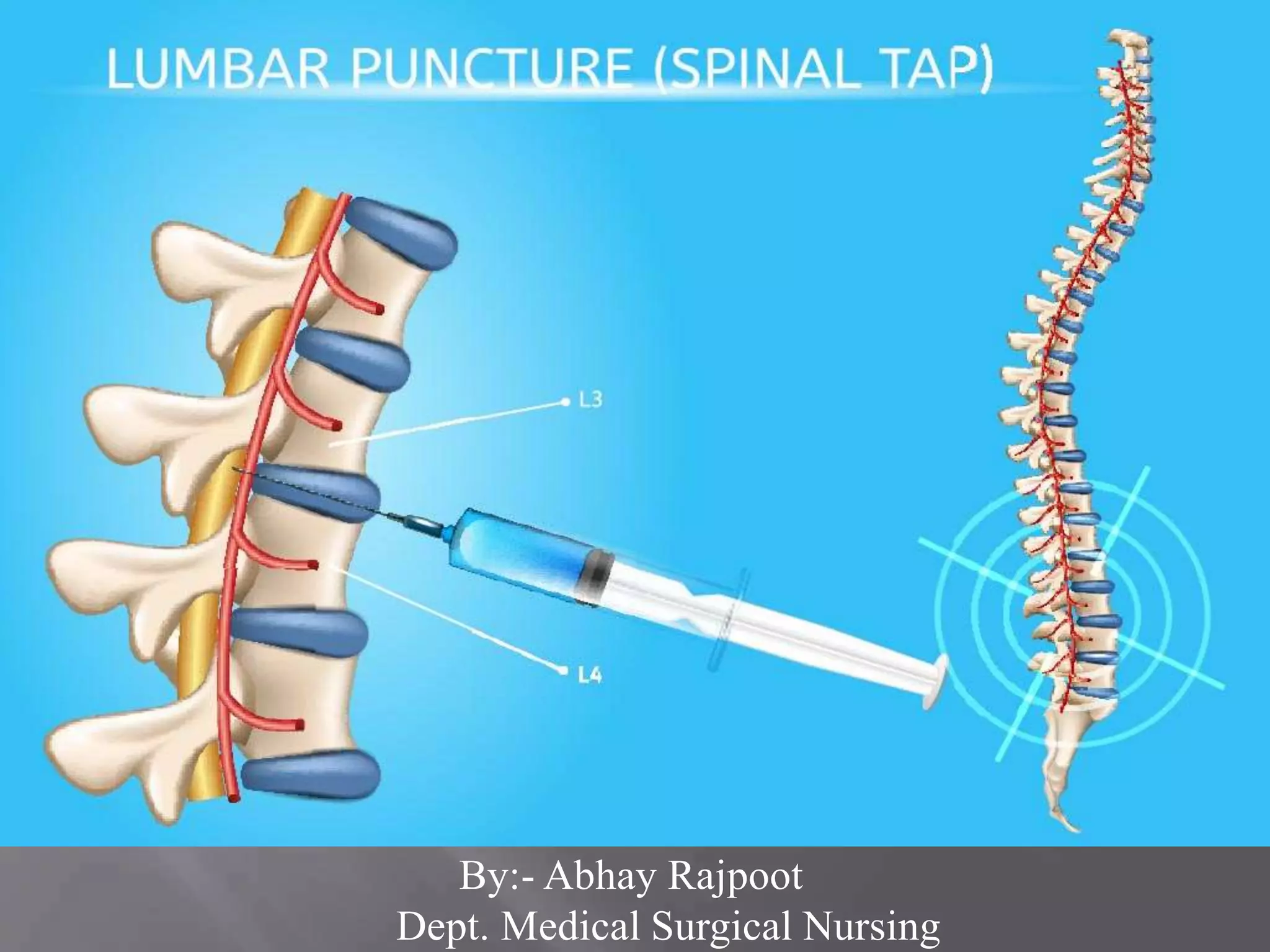
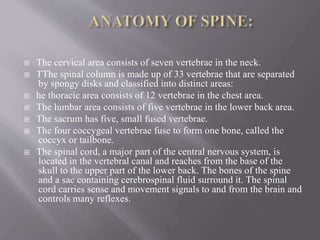
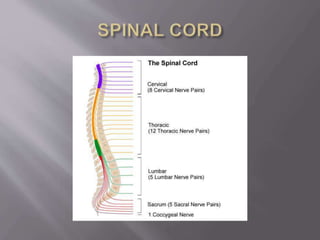


The document provides a comprehensive overview of lumbar puncture, including spinal anatomy, the procedure's definition, indications, contraindications, and potential complications. It details the steps involved in preparing the patient, conducting the procedure, and post-care recommendations to avoid complications such as headaches and infections. Lumbar puncture is essential for diagnosing various central nervous system disorders by extracting cerebrospinal fluid for analysis.























































































