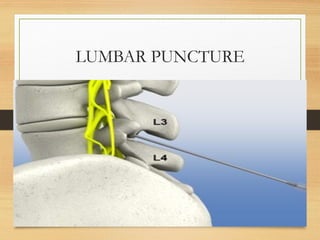
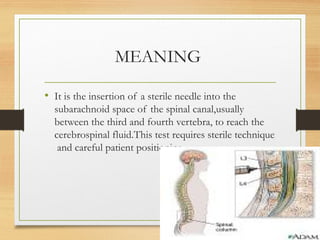
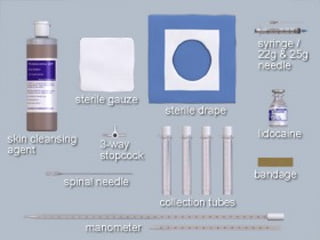
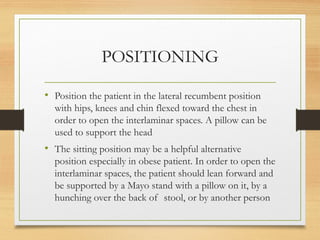
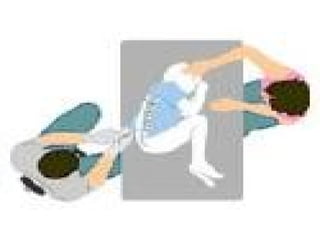
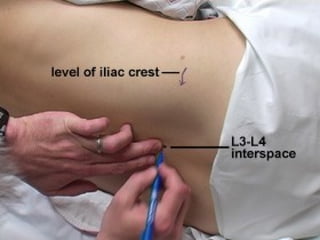
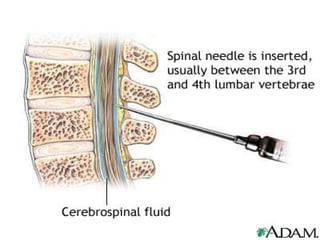
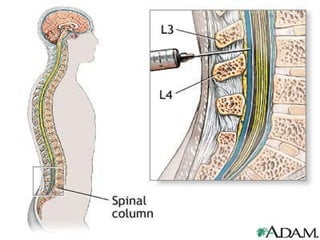
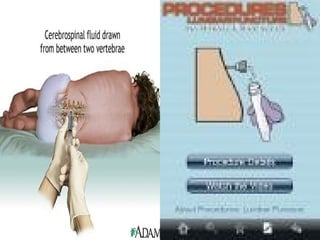
A lumbar puncture involves inserting a sterile needle into the subarachnoid space to collect cerebrospinal fluid for diagnostic purposes, such as detecting infections or other CNS conditions. The procedure requires careful technique, patient positioning, and specific equipment, with considerations for contraindications and complications. Nursing implications include patient education, monitoring for adverse reactions, and ensuring post-procedure care to minimize complications.