Downloaded 1,397 times














![Turn the machine on (notice the mist produced
by the nebulizer)
10. Offer the nebulizer to the patient, offer
assistance until he is able to perform proper
inhalation (if unable to hold the nebulizer
[pediatric/geriatric/special cases], replace the
mouthpiece with mask.](https://image.slidesharecdn.com/nebulization-180710132140/85/Nebulization-23-320.jpg)







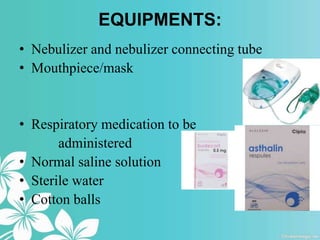
Nebulization is a process that turns liquid medications into mist that can be inhaled into the lungs. It is used to relieve respiratory issues like asthma attacks by delivering medication directly to the lungs. A nebulizer uses compressed air or ultrasonic power to turn liquid medications into a fine mist that patients inhale through a mouthpiece or mask. Proper positioning, instruction on inhalation technique, and monitoring for side effects are important for effective nebulization treatment.









































































