Cystic neoplasm of pancreas
•Download as PPTX, PDF•
3 likes•588 views

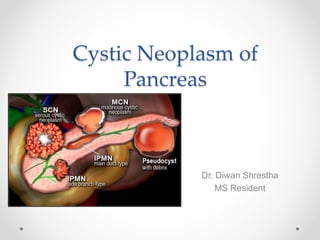
Cystic neoplasms of the pancreas are relatively rare tumors that can be divided into four main types: serous cystic neoplasms (SCN), mucinous cystic neoplasms (MCN), intraductal papillary mucinous neoplasms (IPMN), and solid pseudopapillary neoplasms. SCNs are usually benign and surgical resection is only recommended for large or symptomatic cysts. MCNs and IPMNs have greater malignant potential and surgical resection is generally recommended due to the risk of cancer. IPMNs are further classified as main duct, branch duct, or mixed and location and histological subtype influence malignant risk and management. Surveillance with MRI is recommended post

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Cystic neoplasm of pancreas
Similar to Cystic neoplasm of pancreas (20)
Recently uploaded
Recently uploaded (20)
Cystic neoplasm of pancreas
- 1. Cystic Neoplasm of Pancreas Dr. Diwan Shrestha MS Resident
- 2. Introduction • Second most common exocrine pancreatic neoplasm • Relatively rare neoplasm • 1% of all panceatic neoplasm • 10% of all cystic lesions of pancreas
- 3. WHO classification of pancreatic cystic neoplasms 1. Serous cystic neoplasm (SCN) Serous microcystic adenoma Serous macrocystic adenoma Serous oligocystic adenoma Serous cystadenocarcionoma 2. Mucinous cystic neoplasm (MCN) Mucinous cystadenoma Mucinous cystic neoplasm with moderate dysplasia Mucinous cystadenocarcinoma
- 4. WHO classification of pancreatic cystic neoplasms 3. Intraductal papillary mucinous neoplasm (IPMN) Intraductal papillary mucinous adenoma Intraductal papillary mucinous neoplasm with moderate dysplasia Intraductal papillary mucinous carcinoma 4. Solid pseudopapillary neoplasm Solid pseudopapillary neoplasm Solid pseudopapillary carcinoma
- 5. Types of Cystic Neoplasm • 3 most common type : SCN MCN IPMN • Represent approx 90% of all PCNs • MCN & IPMN Have the highest potential for malignant transformation • SCN Almost always benign
- 6. Serous cystic neoplasm • Female to male ratio (3:1) • Average age 62 years • Common in the head of pancreas • Commonly present with vague abdominal pain Less frequently with weight loss and obstructive jaundice • On gross inspection Large, well circumscribed mass • Microscopic examination Multiloculated, glycogen-rich small cysts
- 7. Serous cystic neoplasm • Central calcification with radiating septa giving the sunburst appearance Radiographic sign on CT 10% to 20% of patients • Tumor larger than 4 cm more likely to be symptomatic display a more rapid median growth rate
- 8. Mucinous cystic neoplasm • Most common cystic neoplasms of the pancreas • Common in perimenopausal women • Men rarely affected • Mean age at presentation fifth decade • Typically found in the body and tail of the pancreas • Incidental MCN becoming increasingly common
- 9. Mucinous cystic neoplasm • 50% patients present with vague abdominal pain 30% have palpable abdominal mass • History of pancreatitis may be found in up to 20% of patients • Tumors span the histologic spectrum from benign to invasive carcinomas < 20% MCNs associated with invasive carcinoma • MCNs contain mucin-producing epithelium Identified histologically by the presence of mucin-rich cells and ovarian-like stroma
- 10. Mucinous cystic neoplasm • CT scan Presence of a solitary cyst May have fine septations Surrounded by a rim of calcification • Cross-sectional imaging may not be able to distinguish between benign and malignant MCNs Presence of eggshell calcification Larger tumor size Mural nodule Suggestive of malignancy
- 11. Mucinous cystic neoplasm • FNA with cyst fluid analysis of MCNs demonstrate Mucin-rich aspirate High CEA levels (>192 ng/mL) • MCNs typically have low levels of cyst fluid amylase • Stroma cells stain Estrogen (25-63%) Progesterone ( 50-80%) Alpha-inhibin (50-70%) • Invasive MCNs exhibit Slower growth Less frequent nodal involvement Less aggressive clinical behavior Compared with ductal adenocarcinoma
- 12. Intraductal papillary mucinous neoplasm • First recognised in 1982 by Ohashi • Defined as intraductal, grossly visible epithelial neoplasm of mucin producing cells • Approx 3-5% of all pancreatic tumors • Peak incidence at 60-70 years • More prevalent in males than female
- 13. Intraductal papillary mucinous neoplasm • Can be 3 types : 1. Main duct IPMN Approx 25% of IPMNs Segmental or diffuse dilation of MPD (>5mm) in the absence of other causes of ductal obstruction MPD is mucin filled & tortous Common near the head of pancreas Adjacent pancreas can be fibrotic & firm due to chronic pancreatitis MD-IPMN have a 30% to 50% risk of harboring invasive pancreatic cancer at the time of presentation
- 14. Intraductal papillary mucinous neoplasm 2. Branch duct IPMN Approx 57% of IPMNs Involves dilation of the pancreatic duct side branches that communicate with but do not involve the main pancreatic duct May be focal, involving a single side branch, or multifocal, with multiple cystic lesions throughout the length of the pancreas Occur in slightly younger population Common in uncinate process Less associated with malignancy Grossly appear as grape like structure that are multicystic containing mucin filled ducts Adjacent pancreas usually normal due to non involvement of main pancreatic duct
- 15. Intraductal papillary mucinous neoplasm 3. Mixed type IPMN Approx 18% of IPMNs A side branch IPMN that has extended to involve the main pancreatic duct to a varying degree Meet criteria for both main & branch duct IPMN
- 16. Intraductal papillary mucinous neoplasm • Majority of IPMNs discovered incidentally Mostly asymptomatic • When symptoms do occur Tend to be non specific Unexplained weight loss, abdominal pain, anorexia Jaundice due to mucin obstructing ampulla Obstruction of pancreatic duct can cause pancreatitis
- 18. Intraductal papillary mucinous neoplasm • Triad of Ohashi Bulging ampulla of Vater Mucin secretion from patulous papilla Dilated main pancreatic duct
- 19. Intraductal papillary mucinous neoplasm • IPMNs based on epithelial lining of papillary component categorised into Gastric Intestinal Pancreaticobiliary Oncocytic • Branch duct IPMN mainly of gastric variant • Main duct IPMNs mainly intestinal type
- 20. Intraductal papillary mucinous neoplasm • All cysts with worrisome features on CT or MRI and any cyst larger than 3 cm with or without worrisome features should undergo EUS • All cysts with high-risk features should be resected
- 22. Management Serous cystic neoplasm • Nearly all SCNs are benign • In older or frial patients Conservative approach • Indications for operative management Presence of symptoms Cyst > 4 cm Uncertainty of diagnosis despite appropriate radiological assesment
- 23. Serous cystic neoplasm • Type of surgical resection Based on position of cyst within the pancreas • Can be Anatomic pancreatectomy ( pancreaticoduodenectomy or distal pancreatectomy) Tissue preserving procedure ( segmental central pancreatectomy) • No role for lymphadenectomy or extended resections Due to inherent benign nature
- 24. Mucinous cystic neoplasm • Surgical resection irrespective of location in the pancreas or size • MCN in the head of pancreas Pancreaticoduodenectomy • MCN in the body & tail of pancreas Distal pancreatectomy • Concurrent splenectomy controversial • Lymph node excision limited to immediate proximity of pancreatic lesion
- 25. Intraductal papillary mucinous neoplasm • IPMN localised to body & tail Distal pancreatectomy with splenectomy • IPMN localised to head or uncinate process pancreaticoduodenectomy
- 28. Intraductal papillary mucinous neoplasm • Endoscopic cyst ablation using ethanol or in combination with Paclitaxel can be done • Ablation can be done for Small cysts Patients with serous comorbidities • Endoscopic ablation with ethanol contraindicated in main duct IPMN Due to interaction of ethanol with the activation of zymogens resulting in acute pancreatitis
- 29. Adjuvant therapy • Patients with evidence of invasive disease on final pathology even in the absence of positive margins • Gemcitabine based chemotherapy with radiotherapy
- 30. Surveillance • Modality of choice MRI • CEA & CA 19-9 has limited role for detection of IPMN recurrence
- 31. THANK YOU