Downloaded 21 times



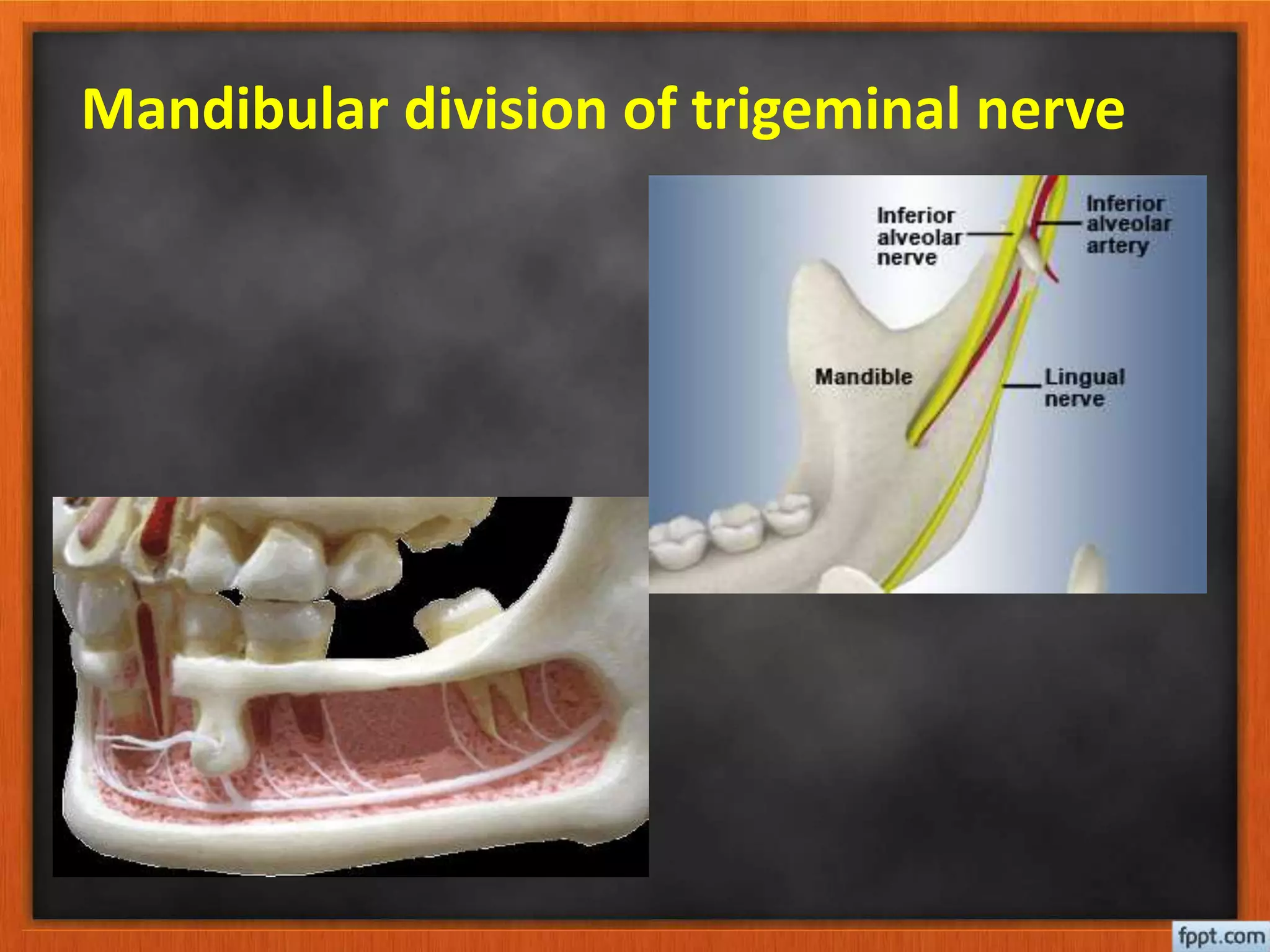

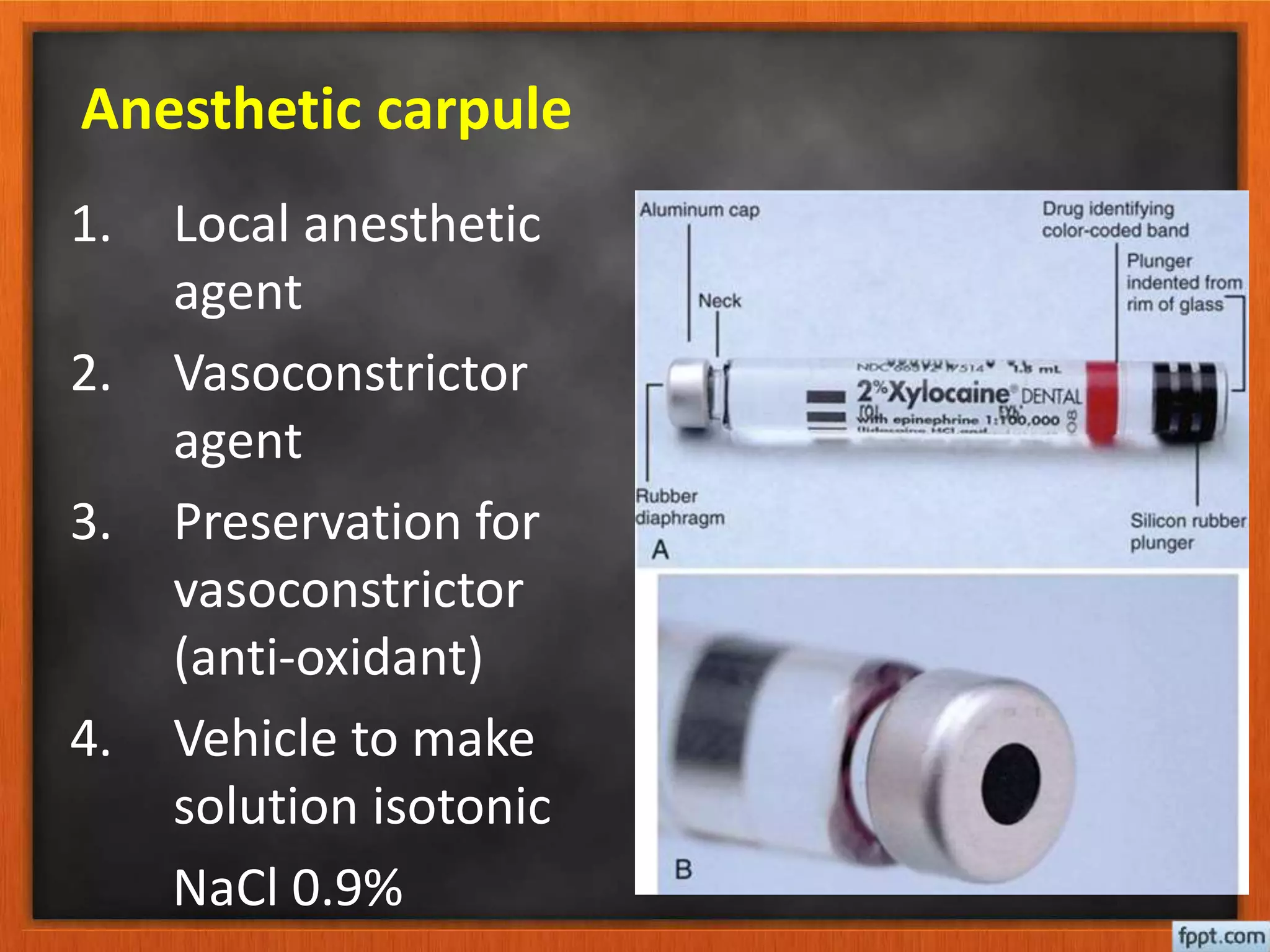























This document discusses local anesthesia techniques for dental procedures. It begins by outlining the importance of local anesthesia and describing local anesthetic agents. It then reviews the anatomy of the trigeminal nerve and its branches. The rest of the document describes various local anesthesia injection techniques for the maxilla and mandible, including infiltration, nerve blocks of the greater palatine nerve, nasopalatine nerve, inferior alveolar nerve, and mental nerve. Proper needle placement, angulation, dosage, and administration technique are emphasized for each injection.



















































![lec 14 [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/lec14autosaved-230315142106-831cdef1-thumbnail.jpg?width=640&height=640&fit=bounds)


































