Downloaded 11 times





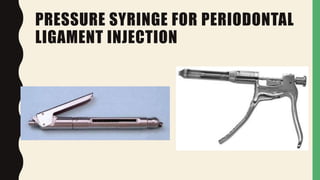

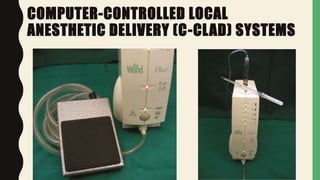
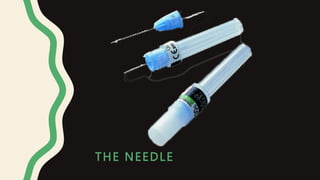
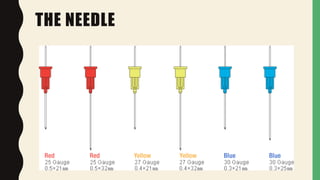
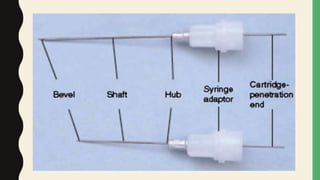
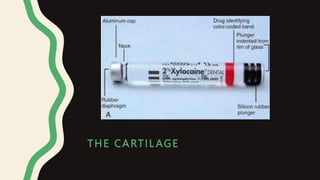

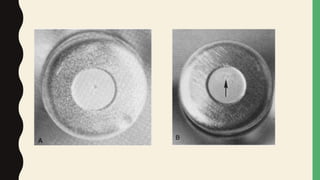









This document discusses local anesthesia equipment and techniques. It describes different types of syringes used to administer local anesthetics including non-disposable, disposable, safety, and computer-controlled syringes. It also discusses dental needles in terms of gauge, length, and potential clinical problems. The dental cartridge components and potential issues are explained. Topical anesthetics are recommended to be applied before needle penetration to minimize pain.

![lec 14 [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/lec14autosaved-230315142106-831cdef1-thumbnail.jpg?width=640&height=640&fit=bounds)