The document discusses the inferior alveolar nerve block technique used in dental procedures. It describes the anatomy of the inferior alveolar nerve, landmarks for the technique, and proper administration methods. Complications can include inadequate anesthesia or lingual numbness. Reasons for failure include anatomical variations, thick mandibular bone, pulpal inflammation, or accessory innervation from other nerves. Alternatives like mental or incisive nerve blocks may provide anesthesia when inferior alveolar nerve block fails.









![Studies have shown the patients who are more anxious prior to the procedure; experience a
higher amount of pain.
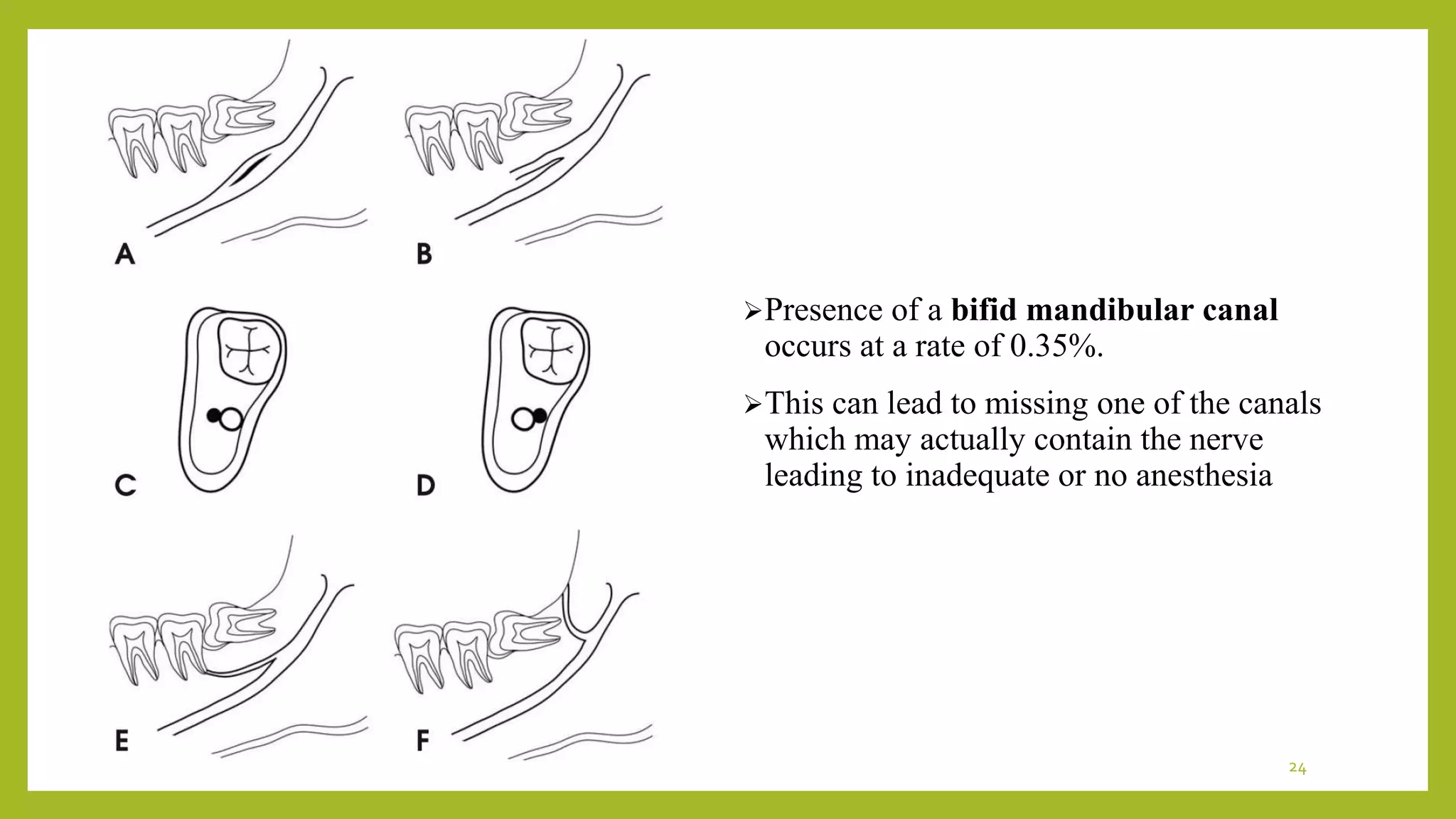
The mandibular hard tissue and soft tissue is supplied by a plexus of nerves. This plexus,
may allow sensation even if primary inferior alveolar nerve is blocked. In 1020% of the
cases, Mylohyoid nerve provides accessory innervation to mandibular molars
TYPE OF ANESTHETIC SOLUTION USED- Cohen et al. showed that 3% mepivacaine
is as effective as 2% lidocaine with 1:100 000 epinepthrine in achieving pulpal anaesthesia
with IANB.
Pulpal inflammation and abscess is a major problem when introducing anesthesia.[11]
Studies have shown changes in the impulse generation of nerve fibres in presence of
inflammation and also suggest changes in peripheral sensory fibers in presence of
inflammation.
23](https://image.slidesharecdn.com/inferioralveolarnerve-200926084113/75/Inferior-alveolar-nerve-23-2048.jpg)