Download to read offline






































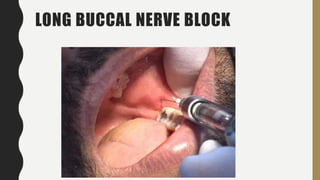


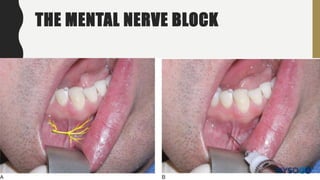
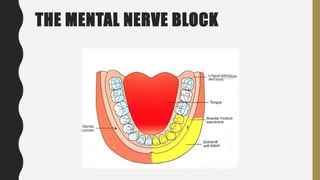

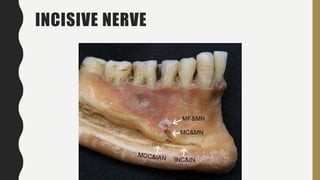













This document discusses techniques for local anesthesia in dentistry. It describes four main types of local anesthesia: topical, infiltration, field block, and regional block. Infiltration anesthesia involves depositing the anesthetic solution near terminal nerve fibers to infiltrate the tissue and anesthetize a localized area. It is commonly used for the front of the maxilla and mandible. Regional block anesthesia deposits the solution near the main nerve trunk to anesthetize a larger area. The document provides details on specific infiltration and regional block techniques for anesthetizing different areas of the maxilla and palate.











































![Techniques of local anesthesia [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/techniquesoflocalanesthesiaautosaved-210618141111-thumbnail.jpg?width=640&height=640&fit=bounds)







![lec 14 [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/lec14autosaved-230315142106-831cdef1-thumbnail.jpg?width=640&height=640&fit=bounds)