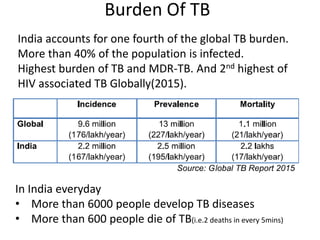
- Tuberculosis is an infectious disease caused predominantly by Mycobacterium tuberculosis that commonly affects the lungs but can affect any part of the body. India accounts for one fourth of the global TB burden with over 6000 new cases and 600 deaths daily.
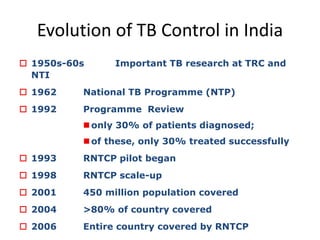
- The Revised National Tuberculosis Control Programme was launched in 1997 based on the WHO DOTS strategy and aims to achieve at least 85% cure rates through direct observation of treatment. It utilizes sputum microscopy, culture and drug susceptibility testing, chest x-rays, and more recently molecular diagnostics to detect TB.
- Drug resistant TB including multi-drug resistant TB has emerged as a major challenge for the programme. The Programmatic Management of Drug Resistant TB was