Downloaded 65 times
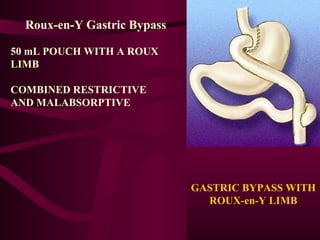
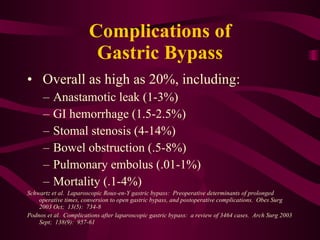



This document discusses potential complications of laparoscopic gastric bypass surgery and provides techniques to address them. It identifies common complications like anastamotic leak, GI hemorrhage, and bowel obstruction. It then outlines steps in the surgical procedure and recommendations to minimize complications, such as properly identifying and dividing tissues, ensuring tension-free anastamoses, and directly testing for leaks. Following surgical principles rigorously and avoiding excessive dissection or suturing can help reduce complications.

































































































