Downloaded 128 times
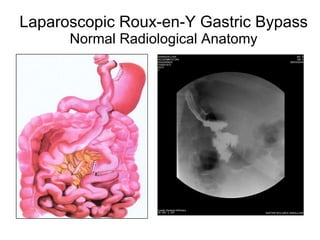

This document discusses complications that can arise after bariatric surgery procedures like Roux-en-Y gastric bypass and adjustable gastric banding. It outlines various early and late technical complications including leakage, bleeding, intestinal obstruction, and band slippage. It also provides case scenarios of patients presenting with abdominal pain, vomiting, or bleeding after these procedures and discusses the evaluation and management of these emergencies, including re-exploration laparoscopy in many cases.
























































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)










