Downloaded 18 times




























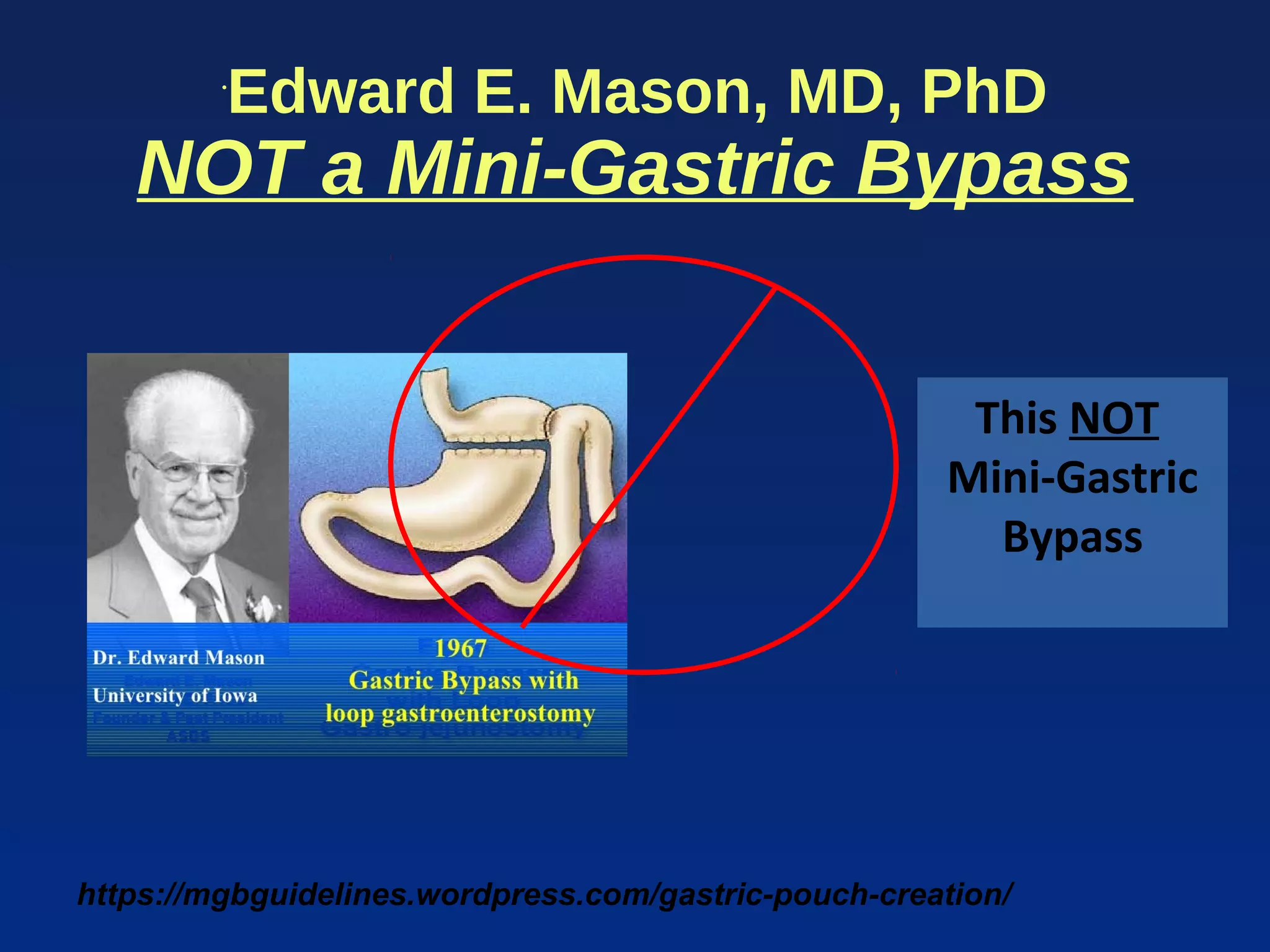



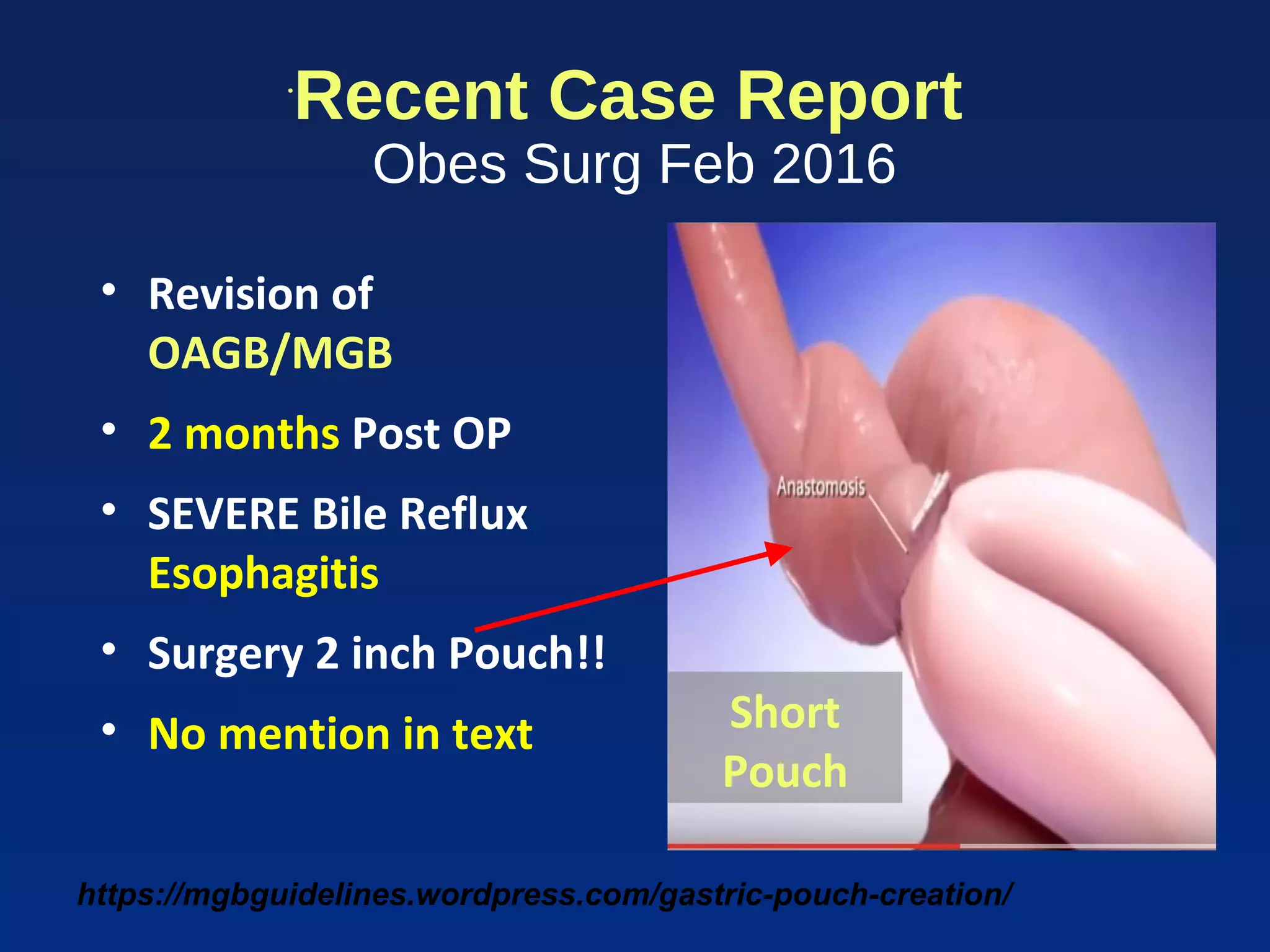









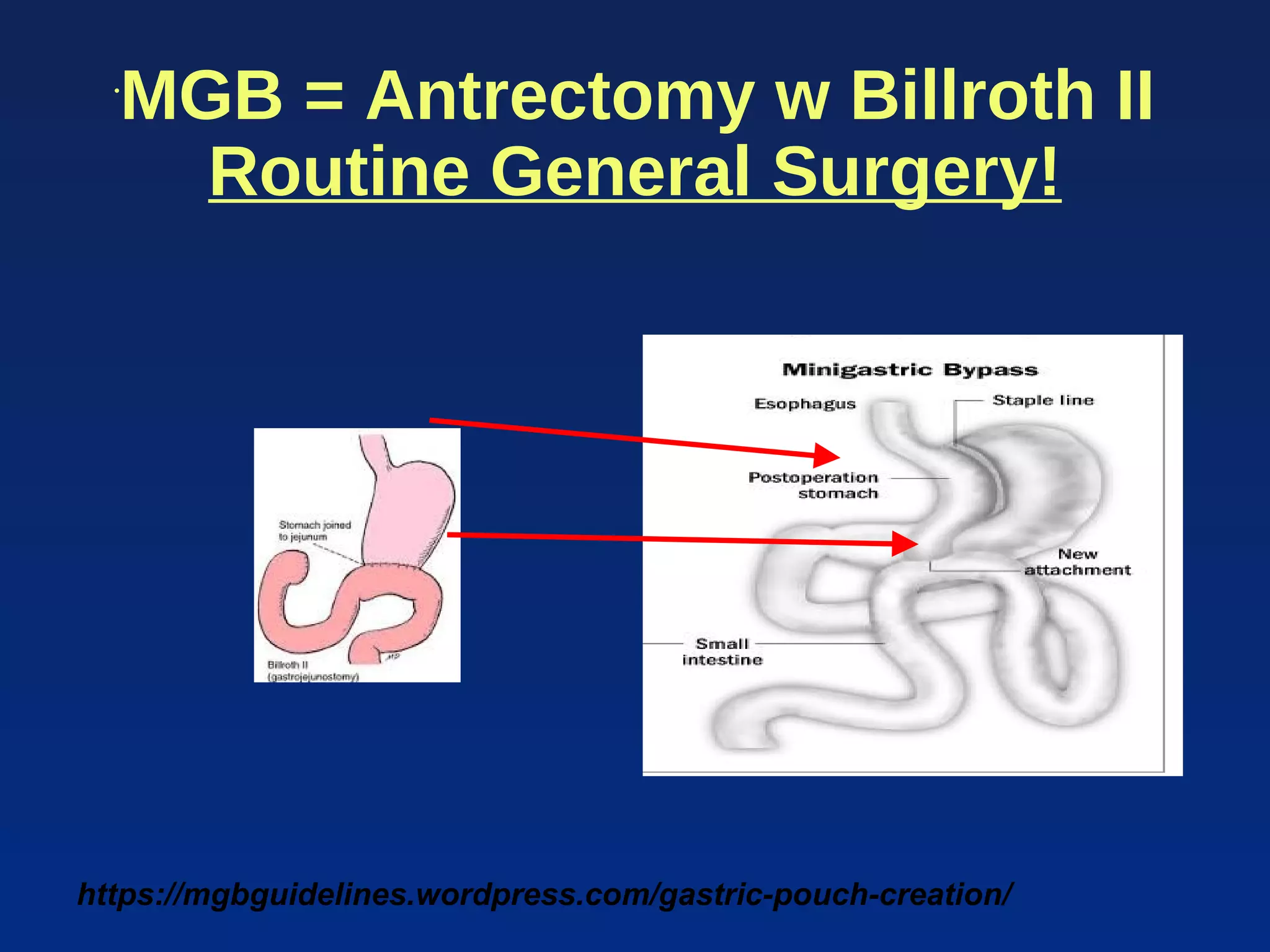
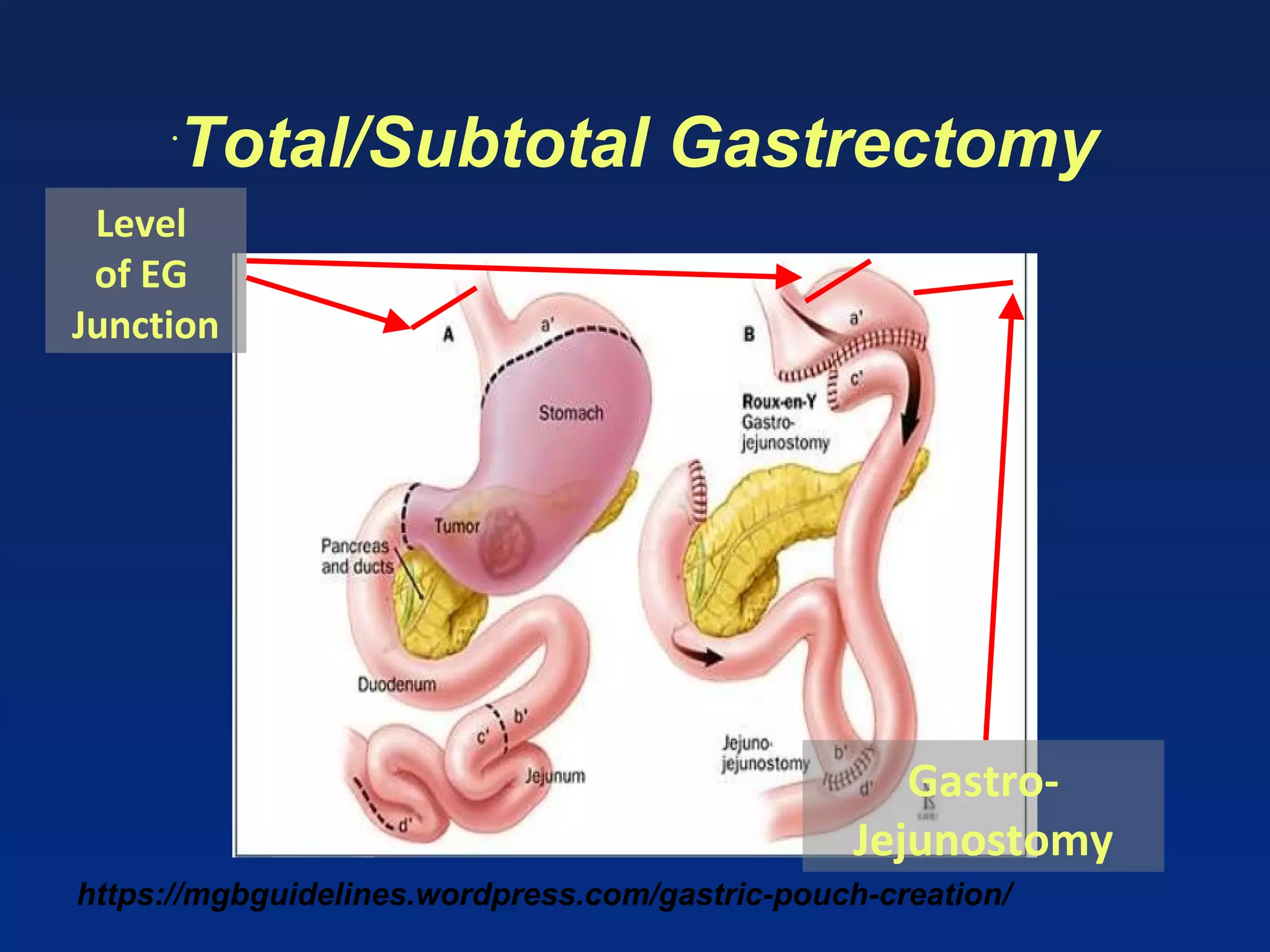

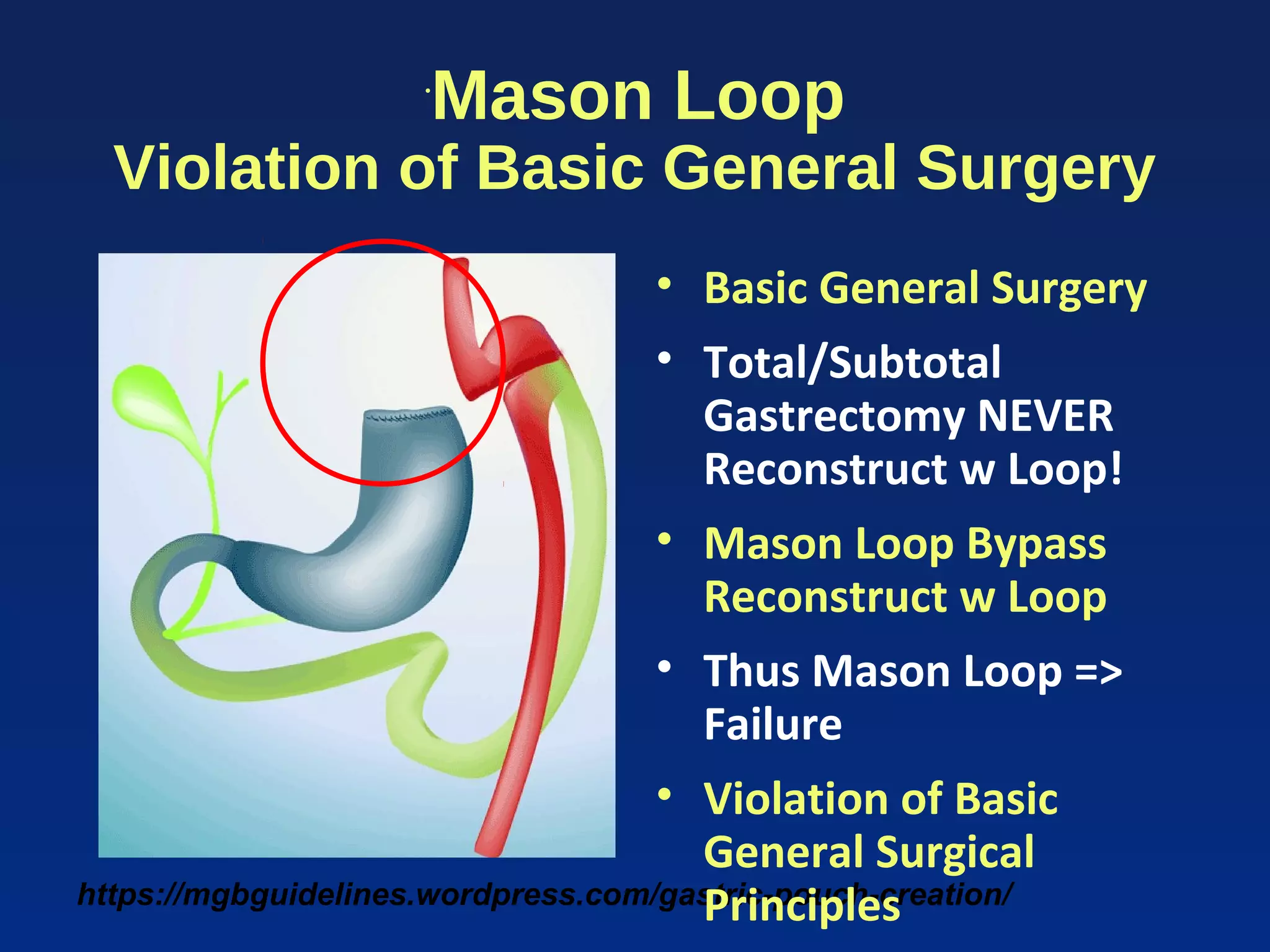













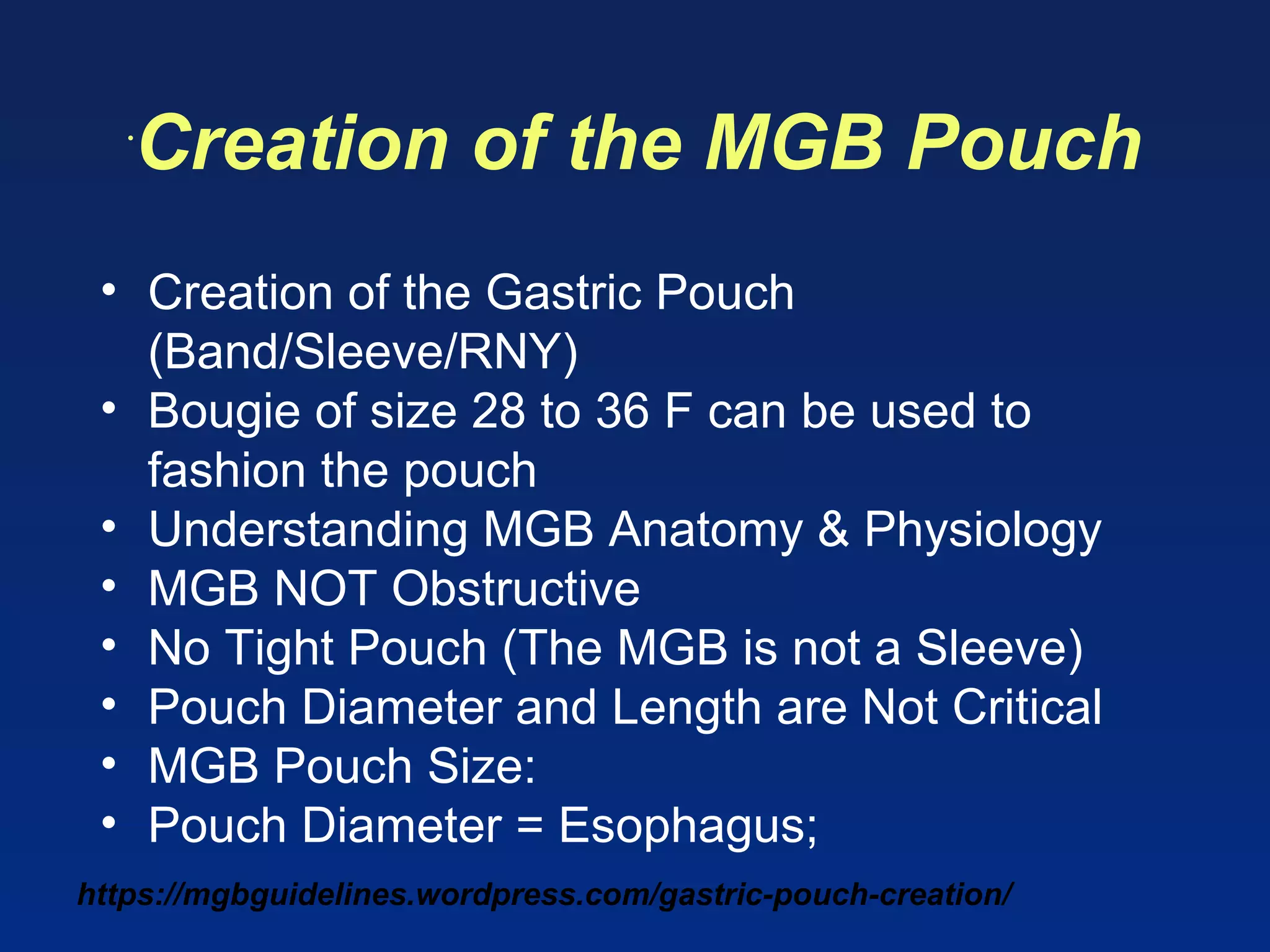




















The document details the mini-gastric bypass (mgb) surgical technique, emphasizing the importance of understanding anatomy and physiology for safe execution. It covers critical steps in creating the gastric pouch and performing gastro-jejunostomy while highlighting the risks of complications from improper practices. Furthermore, it stresses the necessity for education and standardization among surgeons to prevent misunderstandings and improve patient outcomes in mgb procedures.























































































