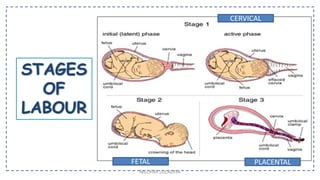
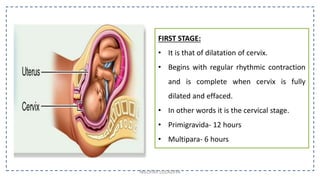
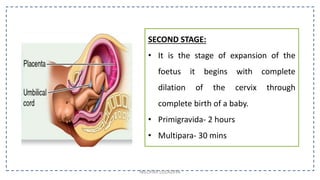
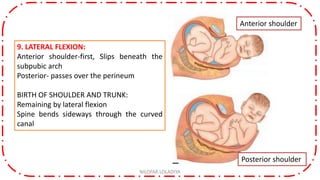
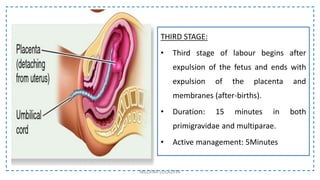
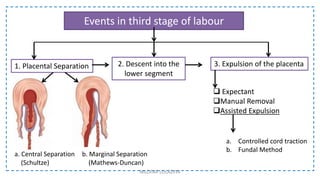
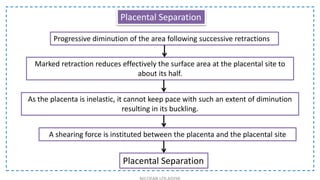
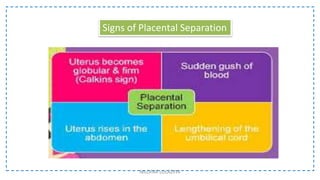
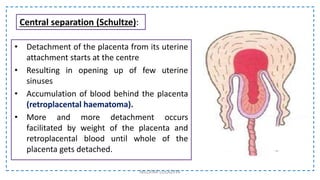
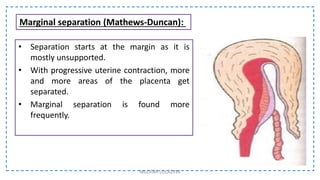
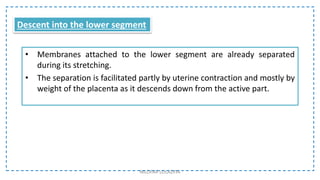
The document provides a comprehensive overview of the stages of labor, detailing the physiological processes during each stage, including first stage dilation, second stage expulsion of the fetus, and third stage expulsion of the placenta. It emphasizes the mechanisms of cervical dilation, uterine contractions, and the critical events that ensure the safe delivery of the fetus and placenta. Clinical management techniques and the importance of hormonal actions during labor are also highlighted.