The document discusses the shift towards preconception care, which reinterprets women's health care as focused on their potential for future pregnancies, often prioritizing the health of potential children over women's current needs. This transformation could lead to reduced quality of care for women, as it risks prioritizing reproductive outcomes at the expense of addressing broader health issues. The author argues that this approach can alienate and coerce women, particularly those not planning to conceive, and may neglect the needs of those outside the reproductive category.
![“ Preconception Care” and the Transformation of Women’s Health Care into Reproductive Medicine Rebecca Kukla Professor of Philosophy and Obstetrics and Gynecology University of South Florida [email_address]](https://image.slidesharecdn.com/kukla-110315072823-phpapp02/85/Preconception-Care-and-the-Transformation-of-Women-s-Health-Care-into-Reproductive-Medicine-1-320.jpg)
![“ Preconception Care” and the Transformation of Women’s Health Care into Reproductive Medicine Rebecca Kukla Professor of Philosophy and Obstetrics and Gynecology University of South Florida [email_address]](https://image.slidesharecdn.com/kukla-110315072823-phpapp02/75/Preconception-Care-and-the-Transformation-of-Women-s-Health-Care-into-Reproductive-Medicine-1-2048.jpg)
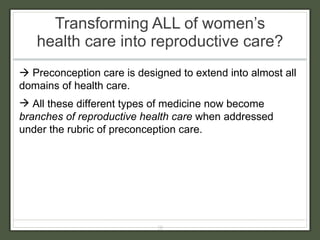
![Transforming ALL of women’s health care into reproductive care? Preconception care is also extending across the lifespan: CDC: “2 nd national summit on preconception health and health care: advancing the health of women and infants before, between, and beyond pregnancy” March of Dimes: Preconception care for girls should begin before adolescence in pediatric clinic. Office of Minority Health: “[Preconception care] starts before birth and it goes from the cradle to the grave.” (??) ASTHO preconception fact sheet: “Preconception care … should take place in an ongoing manner over the course of a woman’s lifespan, beginning in early adolescence, before she is able to become pregnant, and continuing through her reproductive years.”](https://image.slidesharecdn.com/kukla-110315072823-phpapp02/85/Preconception-Care-and-the-Transformation-of-Women-s-Health-Care-into-Reproductive-Medicine-20-320.jpg)